




Pelvic Fractures Can Be Stable & Unstable
- Unstable Fx: a result of high energy trauma with >50% d/t MVA
- 20% closed Fx and 50% of open Fx result in mortality
- Mortality is associated with vascular and internal organs injuries
- Vascular injury: 20% arterial 80% venous
- Chronic morbidity/disability and prolonged pain
- Unstable Fx are rarely seen in the outpatient setting and typically and present to the ED
- Stable pelvic Fx are usually caused by muscles/tendons avulsions and more often seen in pediatric cases
Understanding Pelvic Anatomy Is The Key To Successful Imaging Dx
- The bony pelvis is a continuous ring of bone held by strong ligaments
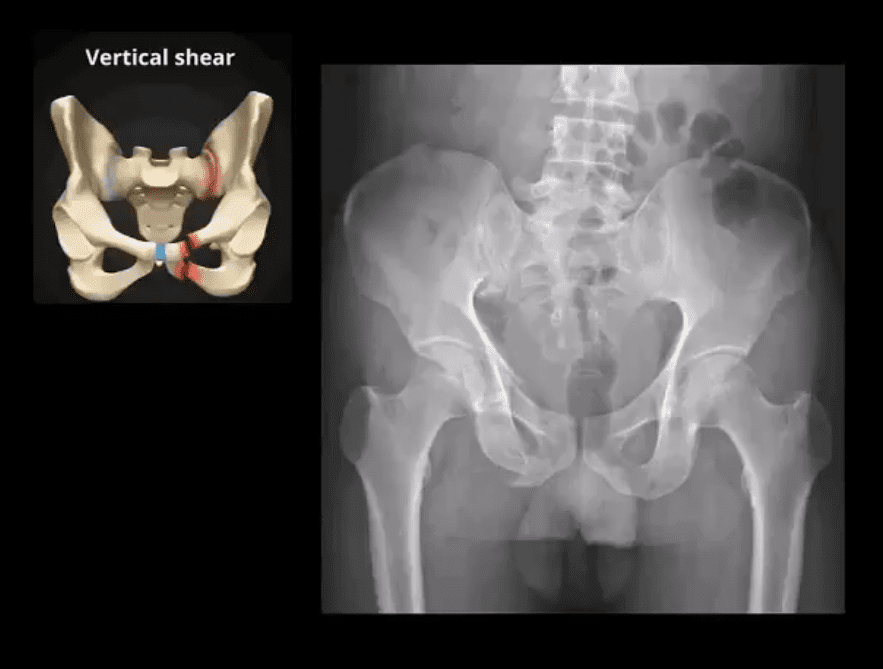
- During significant impact, pelvic fractures may occur in more than one location because forces applied to one region of the ring will also correspond to injury on the other, usually the opposite side of the ring (above image)
- Thus the majority of unstable pelvic Fx will typically demonstrate more than one break
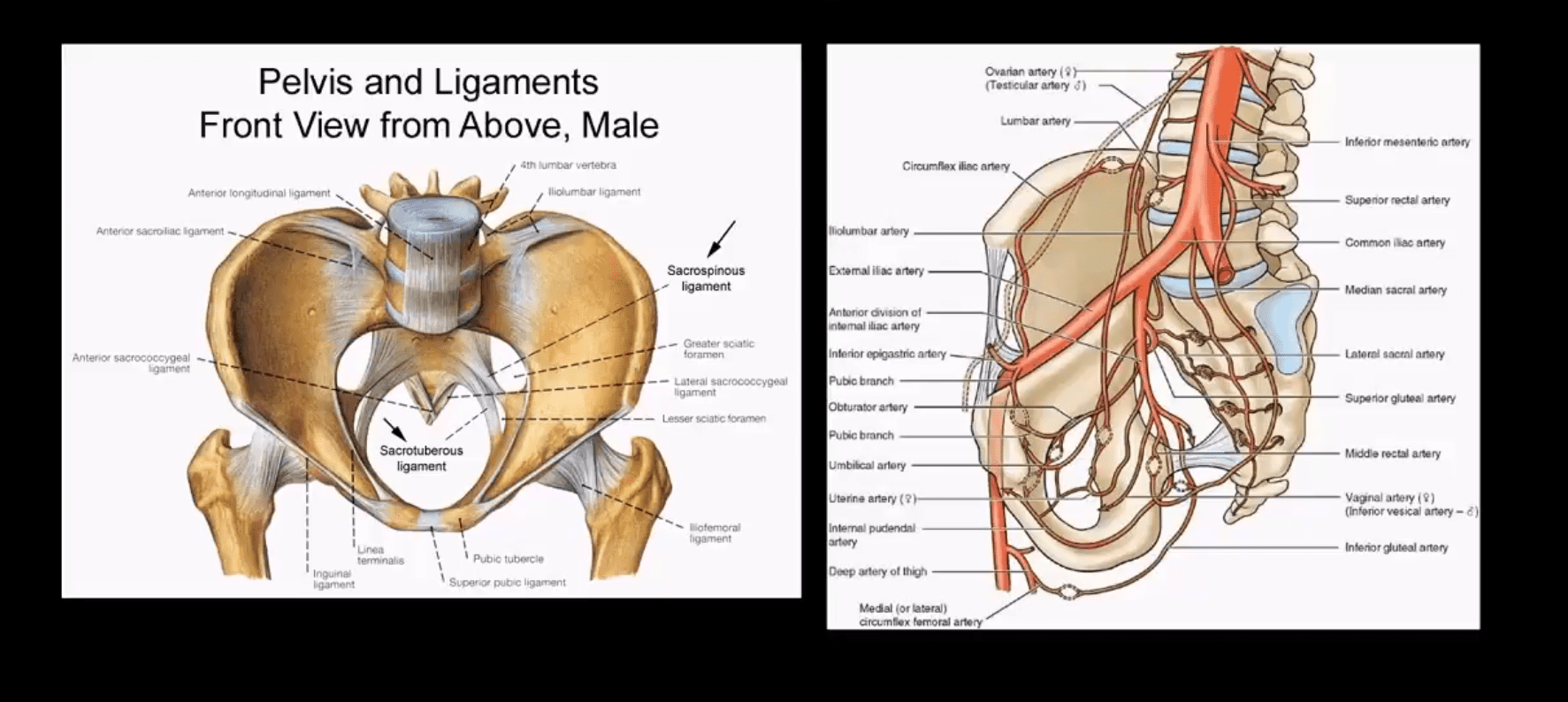
- Pelvic is seen as a ring of bone connected by some of the strongest ligaments in the body
- The pelvic ring comprises 2-semirings: anterior to the acetabulum and posterior to the acetabulum
- The bony pelvis is in close proximity to major vessels carrying a greater chance of vascular injury
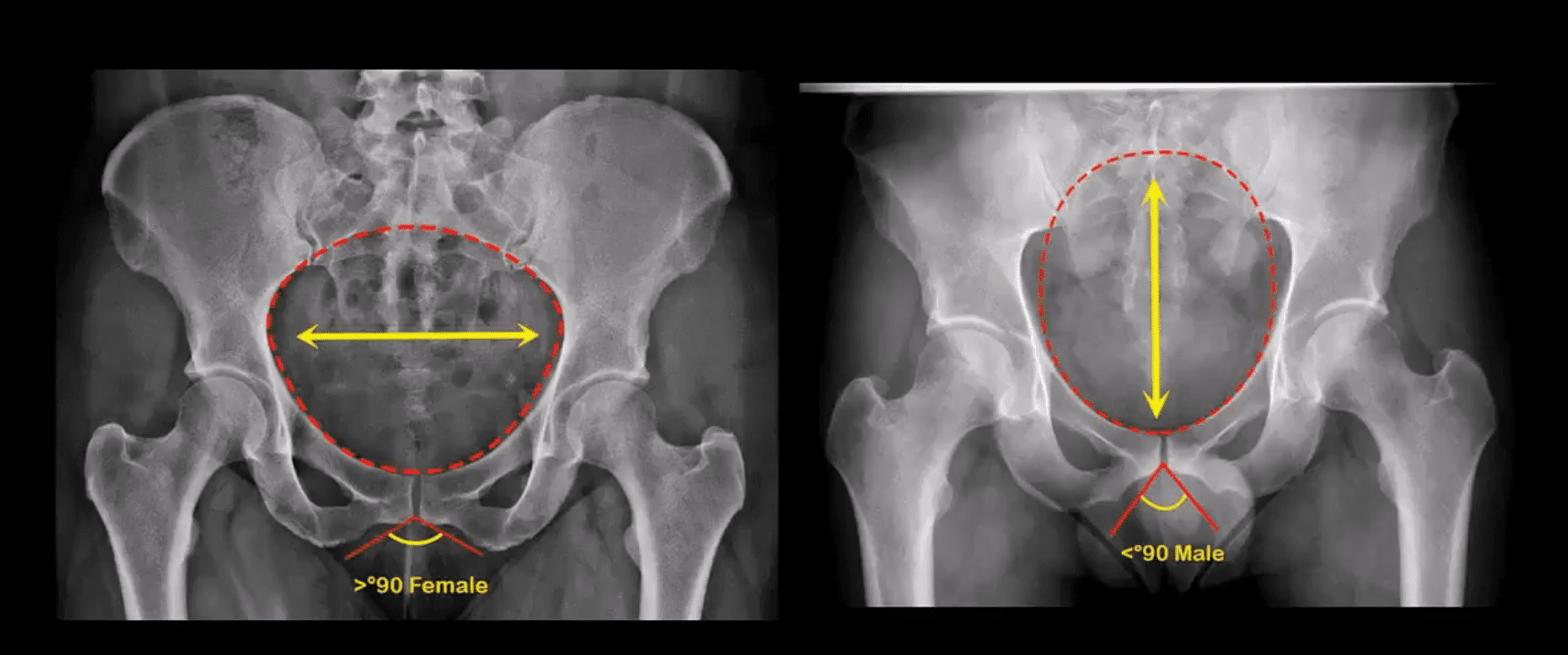
- Anatomical Differences of The Female and Male Pelvis
Post-Traumatic Pelvic Views May Vary and Include:
- Standard AP Pelvis (above images)
- Judet views evaluating the acetabulo-pelvic region
- Inlet/Outlet views helping with the symphysis and SIJ regions
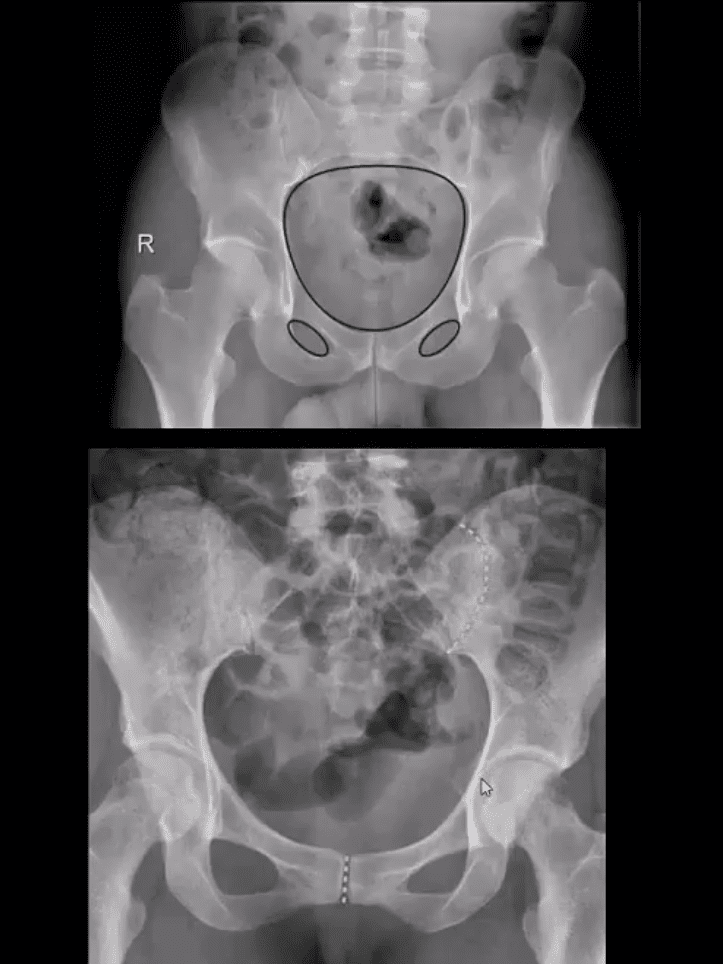
- Rad survey of the pelvis should include evaluation of the continuity of pelvic rings:
- Inlet/outlet, obturator rings (above the first image)
- Symphysis pubis and SIJ for diastasis and post-trauma separation (above the second image)
- Lumbosacral spine and hips should also be carefully examined
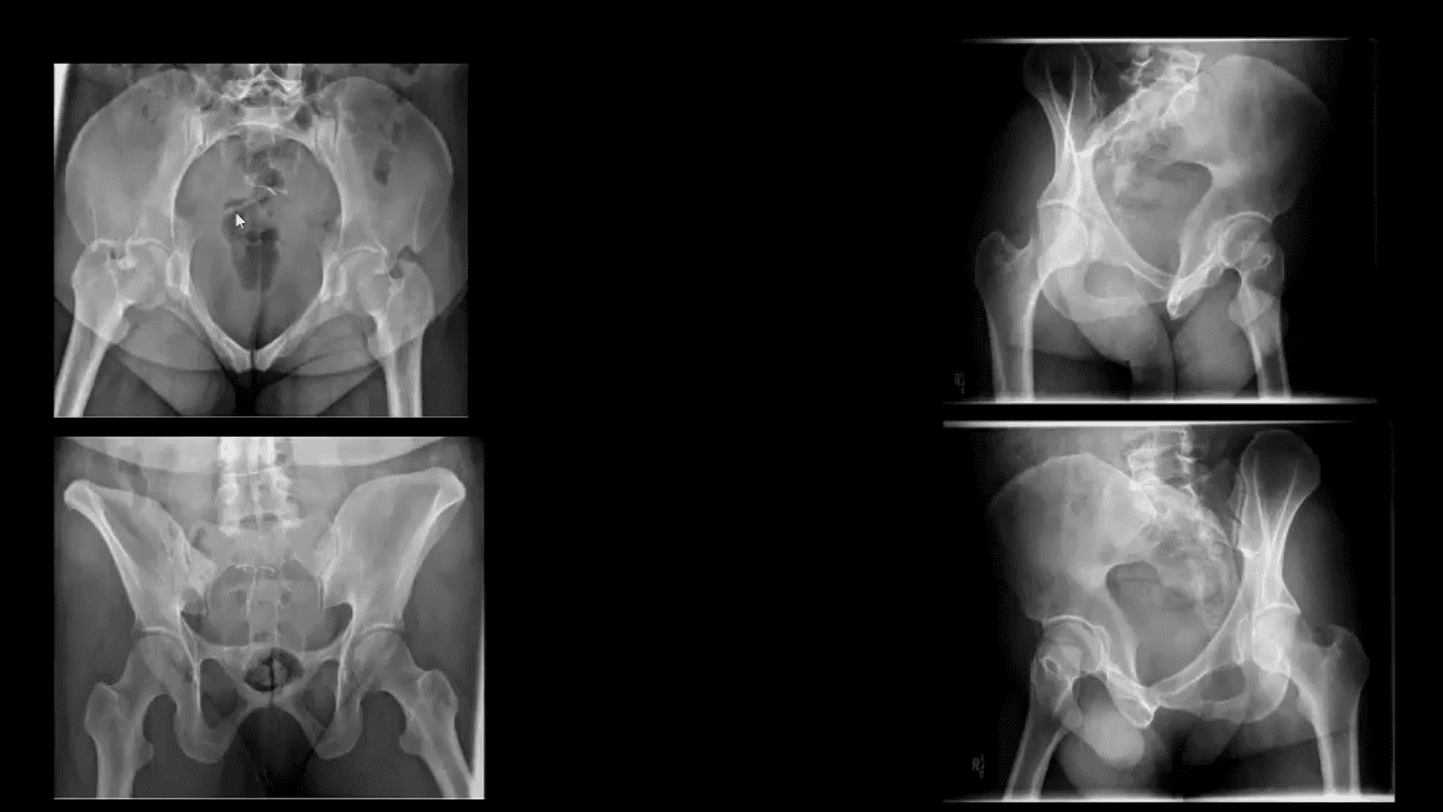
- Pelvic inlet (above top left) and Outlet (above bottom left)
- Judet views: left and right posterior oblique views
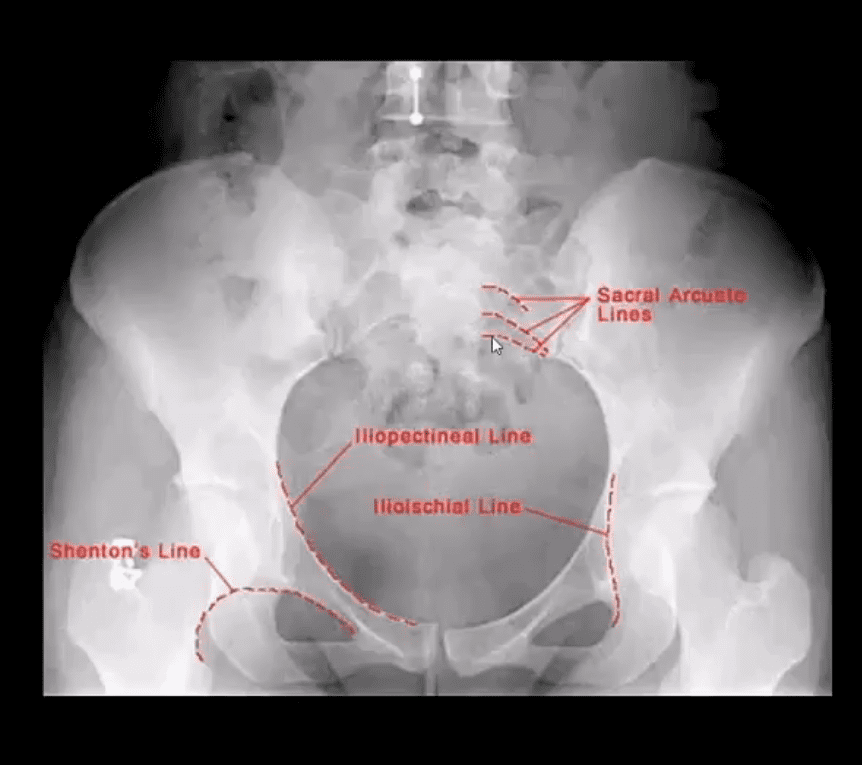
Additional Survey:
- Iliopectineal, ilioischial, Shenton and Sacral arcuate lines will help detection of sacral, acetabular and hip fracture/dislocations
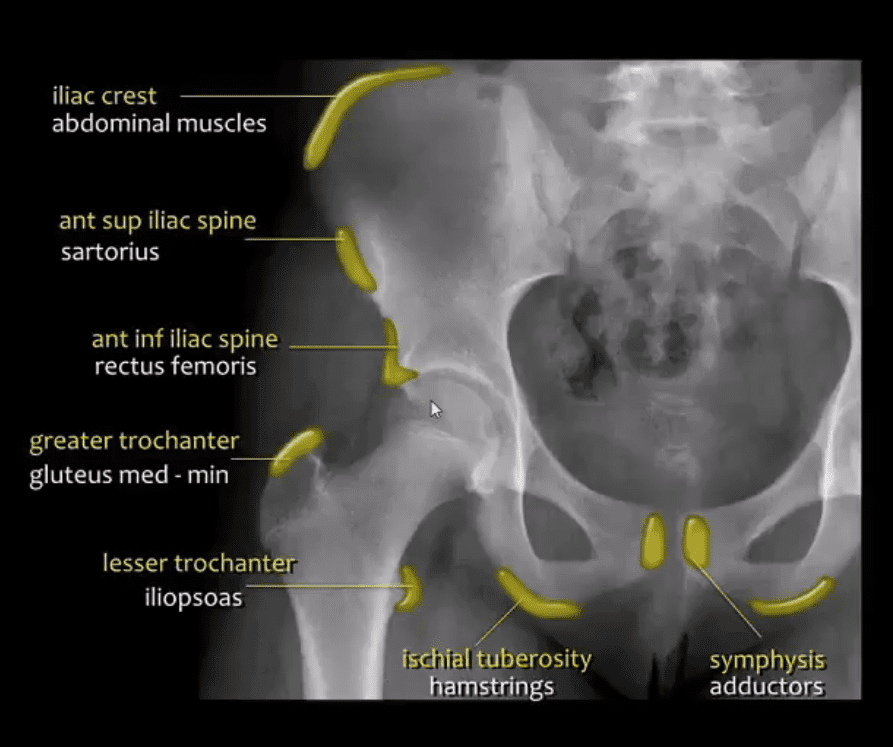
Stable Pelvic Fractures aka Avulsion Injury
- Appreciating anatomical sites of pelvic origin/insertion of different muscles will help Dx of pelvic avulsion Fx
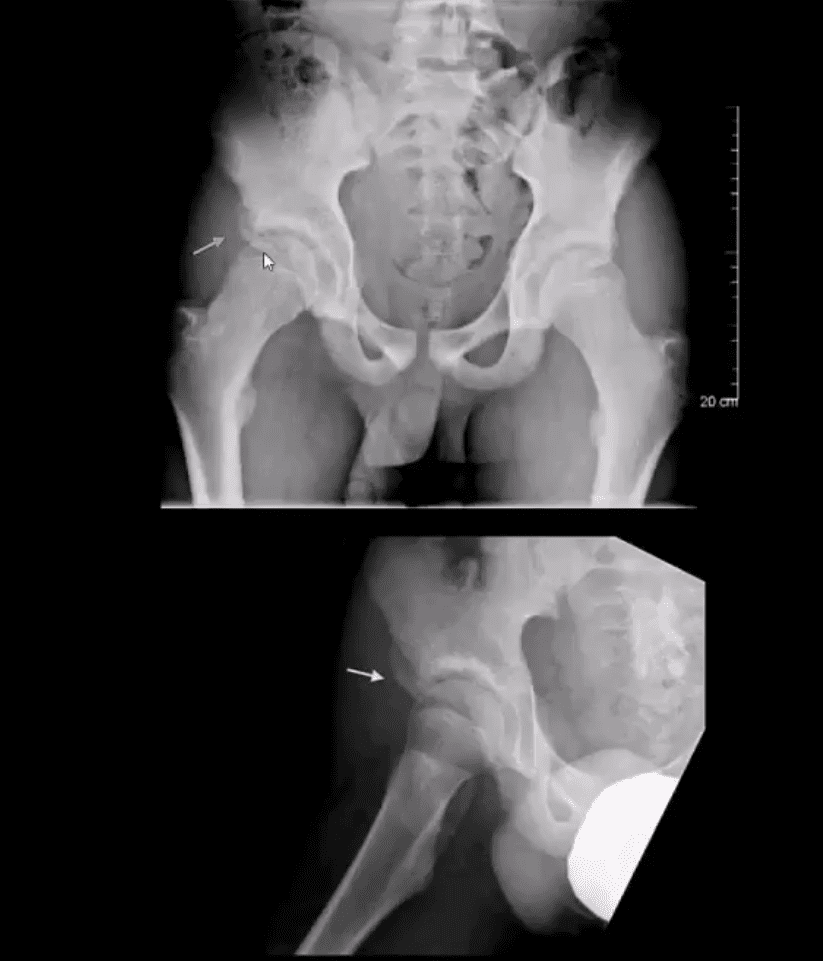
- Avulsion Fx of the AllS (origin of the direct head of Rectus femoris M)
- Pelvic avulsions occur by sudden eccentric contraction especially during kicking or jumping
- Imaging: x-radiography will suffice
- Clinically: sudden snap or pop followed by local pain. Pt can weight bear
- Care: non-operative with rest for 4-weeks. Non-union is rare. No major complications
- DDx: key rad DDx feature is not to mistake an avulsion from an aggressive pediatric bone tumor-like osteosarcoma that may show some exuberant new bone formation d/t healing and bone callus
Commonly Encountered Unstable Pelvic Fractures
- Malgaigne Fx: d/t vertical shear injury to the ipsilateral pelvis
- Rad Dx: ipsilateral superior and inferior pubic rami Fx (anterior ring) with ipsilateral SIJ separation/Fx of the sacrum and adjacent ilium (posterior ring). Symphysis pubis diastasis can be seen. An additional clue is an avulsion of L4 and/or L5 TP that often signifies serious pelvic injury
- Clinically: marked leg shortening, shock, inability to weight bear.
- Damage to Superior Gluteal Artery can occur
- Imaging: x-radiography followed by CT scanning w/o and with IV contrast esp. if visceral injury present
- Care: surgical in most cases d/t significant instability. ORIF. Hemostasis, Pelvic stabilization
- Prognosis: depends on the complexity, rate of visceral complications and stability. 10% Superior glut artery bleed requiring rapid hemostasis
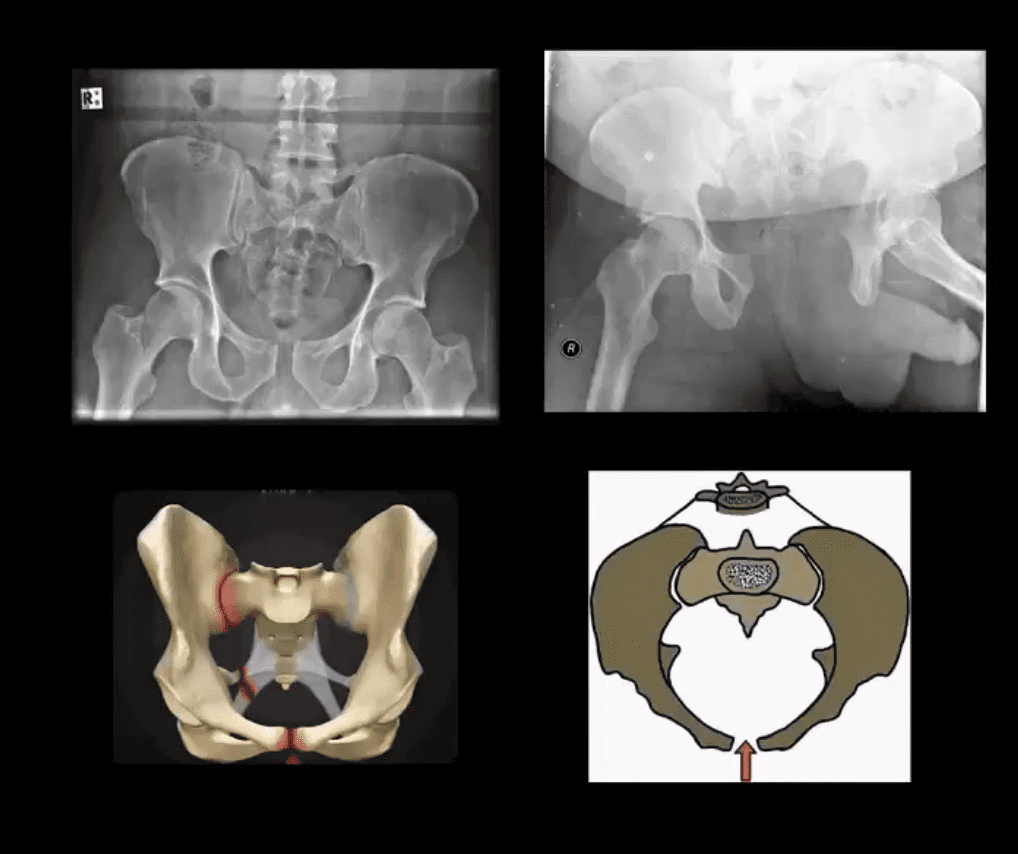
Open Book Pelvis (major instability)
- Mechanism: AP compression of different force magnitude (picture depiction)
- Rad Dx: diastasis of symphysis pubis with diastasis of SIJ with and w/o adjacent Fx of the ala
- Imaging steps: x-radiographic, CT scanning with and w/o contrast for vascular injury, cystography for acute urinary bladder rupture
- Immediate and delayed complications may occur: vascular injury, urethral/bladder injury
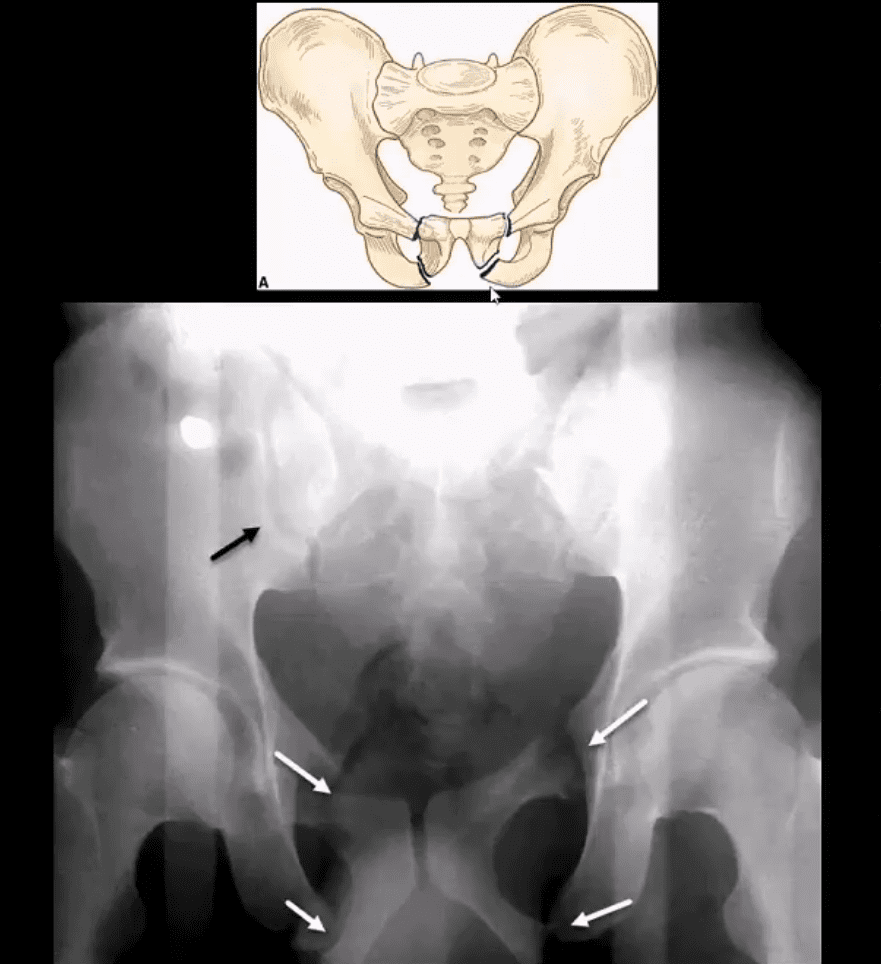
Straddle Injury: Unstable Fx
- Mechanism: direct impact/collision
- High risk of urinary bladder/urethral injury
- Imaging: bilateral superior and inferior pubic rami Fx with or w/o diastasis and Fx of SIJ
- CT with and w/o contrast for vascular injury
- Cystourethrogram additionally evaluates a urogenital injury
- Complications: urethral strictures, bleeding, bladder rupture
- Note: Straddle Fx with right SIJ separation
Hip Fractures (Femoral Neck)
- Common injury
- Occurs in:
- 1) Young adults due to high energy trauma
- 2) Osteoporotic patients with low impact, trivial or no trauma (i.e., insufficiency Fx)
- X-radiography is crucial to early Dx and prevention of complications which include:
- Dx: intra-capsular vs. extra-capsular Fx
- Ischemic osteonecrosis aka avascular necrosis (AVN) of the femoral head and rapid disabling DJD
- Epidemiology: USA has some of the highest rates of OSP hip Fx worldwide. Highest healthcare cost Fx to treat overall
- Women>men, Caucasians>African-Americans
- 25-30% mortality within the 1st year. Mortality depends on co-morbidities and stat of activity prior Fx
- Pathophys: the femoral neck is intra-capsular and transmits arterial flow to the head. The neck is uncovered by the periosteum and unable to develop a good callus. The neck transmits maximum tensile forces through the proximal femur and prone to Fx and non-union
Hip Strengthening
Acute Pelvis & Hip Trauma
