




These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Medial Hamstrings and Adductors
Assessment for shortness in medial hamstrings (semi-membranosus and semi-tendinosus as well as gracilis) and short adductors (pectineus, adductors brevis, magnus and longus)
Method (a) The patient lies so that the non-tested leg is abducted slightly, heel over the end of the table. The leg to be tested is close to the edge of the bed and the practitioner ensures that the tested leg is in its anatomically correct position, knee in full extension and with no external rotation of the leg, which would negate the test.
The practitioner should effectively stand between patient’s leg and the table so that all control of the tested leg is achieved with his lateral (non-table-side) arm/hand, while the table-side hand can rest on and palpate the inner thigh muscles for sensations of bind as it is taken into abduction. Abduction of the tested leg is introduced passively until the first sign of resistance is noted (see Fig. 4.3). Effectively, there are three indicators of this resistance:
- A sense that the motive hand carrying the leg picks up as an increase in required effort at the moment that the first resistance barrier is passed
- The sense of bind noted by the palpating hand at this same moment
- A visual sign, movement of the pelvis as a whole, laterally towards the tested side, as the barrier is passed.
If abduction produces an angle with the mid-line of 45° or more, then no further test is needed, the abduction is normal, and there is probably no shortness in the short or long adductors (medial hamstrings or, more correctly, gracilis and biceps femoris). If, however, abduction ceases before a 45° angle is easily achieved (without effort or a sense of bind in the tissues), then restriction exists in either the medial hamstrings or the short adductors of the thigh.
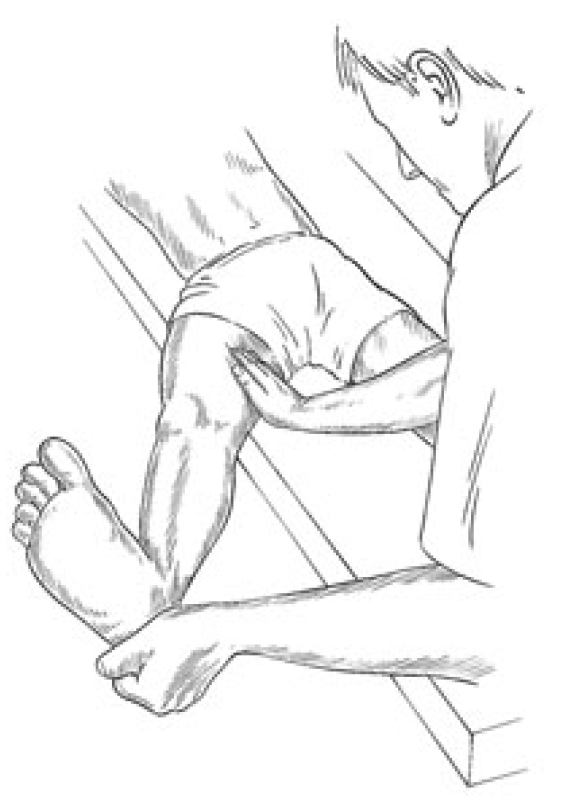
Figure 4.3 Assessment and treatment position for medial hamstrings. Adductor shortness may be evaluated and treated in the same relative position but with the knee of the leg to be treated in flexion.
Screening Short Adductors from Medial Hamstrings
As in the tests for gastrocnemius and soleus, it is necessary to screen between shortness of the one and two joint muscles (in this case the short adductors and the medial hamstrings). This is achieved by abducting the leg to its easy barrier and then introducing flexion of the knee, allowing the lower leg to hang down freely.
If (after knee flexion has been introduced) further abduction is now easily achieved to 45°, this indicates that any previous limitation into abduction was the result of medial hamstring shortness, since this is no longer operating once the knee has been flexed. If, however, restriction remains (as evidenced by continued ‘bind’ or obvious restriction in movement towards allowing a 45° excursion once knee flexion has been introduced to the abducted leg), then it is apparent that the short adductors are continuing to prevent movement, and are short.
Assessing for shortness in medial hamstring (03) /short adductors (04)
Method (b) The patient lies at the very end of table (coccyx close to edge), non-tested leg fully flexed at hip and knee and held to chest by patient (or sole of patient’s foot resting against practitioner’s lateral chest wall) to stabilise pelvis in full rotation, so that the lumbar spine is not in extension. Tested leg is grasped both above and below the knee and taken into abduction to the first sign of resistance. The practitioner has two free hands in this position, one of which can usefully palpate the inner thigh for bind during the assessment.
If abduction reaches 45°, then the test has revealed no shortness. If a restriction/resistance barrier is noted before 45°, then the knee should be flexed to screen the short adductors from the medial hamstrings as in method (a) above. In all other ways the findings are interpreted as above.
MET Treatment of Shortness in Short and Long Adductors of the Thigh
Precisely the same positions may be adopted for treatment as for testing, whether test method (a) or test method (b) was used. If the short adductors (pectineus, adductors brevis, magnus and longus) are being treated, then the leg, with knee flexed, is held at the barrier (acute) or a little short of the barrier (chronic).
An isometric contraction is introduced by the patient using around 20% of available strength (longer and somewhat stronger for chronic than acute) employing the agonists (the push is away from the barrier of resistance) or the antagonists (the push is towards the barrier of resistance) for 7–10 seconds. Appropriate breathing instructions should be given (see notes on breathing in Box 4.2).
After the contraction ceases and the patient has relaxed, the leg is eased to its new barrier (if acute) or painlessly (assisted by the patient) beyond the new barrier and into stretch (if chronic), where it is held for not less than 10 seconds (longer if possible), in order to stretch shortened tissue. The process is repeated at least once more.
If the medial hamstrings (semi-membranosus, semi-tendinosus as well as gracilis) are being treated, all elements are the same, except that the leg should be held in extension, with no bend of the knee (Fig. 4.4).
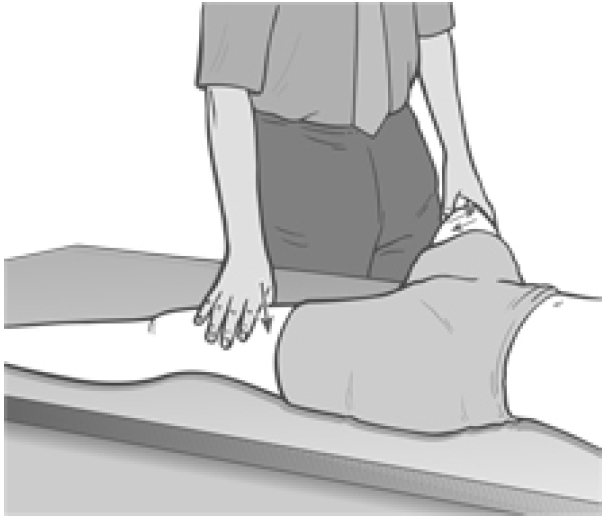
Figure 4.4 Position for treatment of shortness in adductors of the thigh.
Whichever position is used, the subsequent stretch, on an exhalation, is used to (acute) or through (chronic) the barrier to commence normalisation of the short muscles.
Caution and Alternative Treatment Position (Fig. 4.5)
The major error made in treating these particular muscles using MET relates to allowing a pivoting of the pelvis and a low spinal sidebend to occur. Maintenance of the pelvis in a stable position is vital, and this can most easily be achieved via suitable straps or, during treatment, by having the patient side-lying with the affected side uppermost.
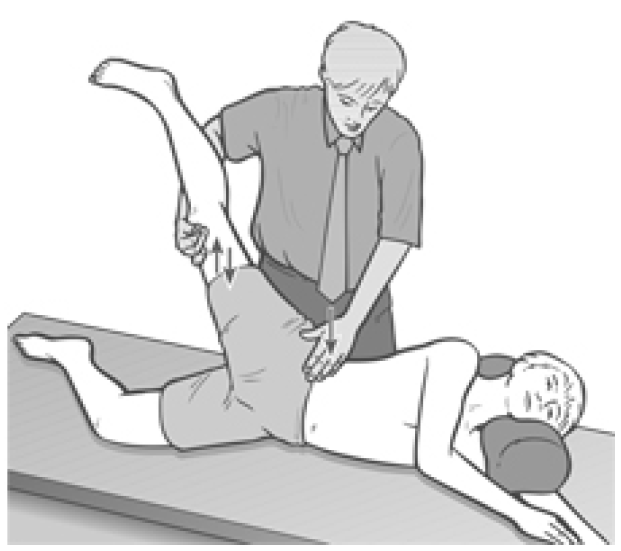
Figure 4.5 Sidelying position for treatment of two-joint adductors of the thigh.
Method (c) Patient is side-lying. Practitioner stands behind and uses the caudad arm and hand to control the leg and to palpate for bind, with the treated leg flexed or straight as appropriate. The cephalad hand maintains a firm downwards pressure on the lateral pelvis to ensure stability during stretching. All other elements of treatment are identical to those described for supine treatment above.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez

Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.

