




Wrist injuries are discussed by Chiropractor, Dr. Alexander Jimenez, with emphasis on the participation of the bone capitate, and how you can modify your training with a wrist injury.
Wrist injuries are underestimated within sport; however, they could account for between 3-9 percent of all athletic injuries (1). Injury can occur from repetitive overuse, or can occur from a single traumatic event, such as falling on an outstretched hand, or impact from a ball or racquet. Regardless of whether it is directly used, the wrist is vulnerable to injury in any sport.
The wrist joint is not supposed to withstand weight bearing or heavy loads like the joint is tight also, though these joints are often thought of in a manner due to the size and distal origin of those limbs. Regardless of this, exercises and many sports involve weight bearing through the wrists or higher impact directed to the joints, ie gymnastics, racquet and hand ball sports, strength training including press-ups, boards, and yoga poses. Sports played hard surfaces can also traumatize the wrist since the body weight of the athlete can land upon the joint, and the difficult surface (astro turf, ice, or racquet court will not absorb the shock as much as a forgiving ground surface). These activities all require wrist extension (the bending of the wrist backwards) and also pain from this is often localized to the dorsal surface (rear of this hand/wrist). Because they are the most commonly encountered this guide will focus on extension accidents.
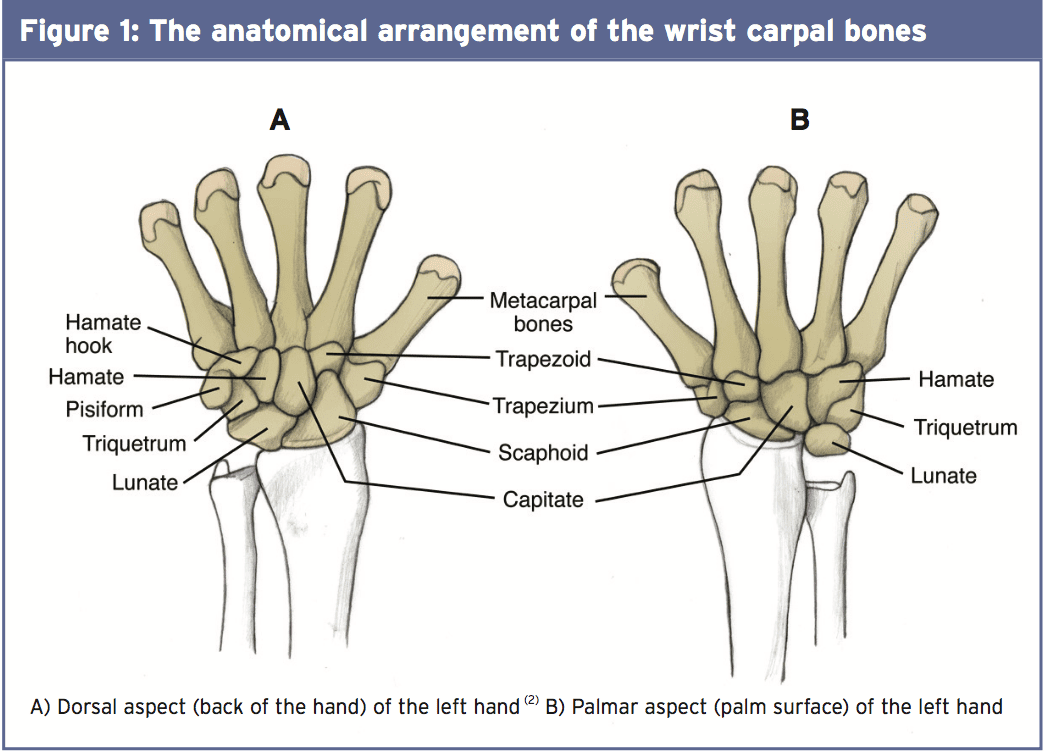
The “wrist joint” is more anatomically called the radiocarpal joint. This is the connection between the radius (forearm bone) and the proximal row (closest to the forearm, where the wrist crease happens) from the cervical bones. The main job of the radiocarpal joint is to allow motion of the hand upward (extension) and back (flexion). This can be stabilized by the radioulnar ligaments which connect ulna forearm bones and the radius anteriorly and posteriorly.
The bones are then divided into two rows. The proximal row consists from lateral (external nearest the thumb) into medial of scaphoid, lunate, triquetrum, and pisiform. The row is made up of trapezium, trapezoid, capitate, and hamate. Various small ligaments join the carpal bones into each other, permitting fine motions around each other whilst being kept securely in position(3). These connections allow the wrist to have the fine motor control that tasks demand, in addition to the power for heavy gripping tasks.
The wrist joint is capable of roughly 85 degrees of wrist flexion and extension, and this movement happens at the radiocarpal joint and the midcarpal joint (between the proximal and distal rows). It can also move side to side with 15 degrees of radial deviation (towards the thumb) and 45 degrees of ulnar deviation (towards the fifth finger)(2).) These movements again result from the radiocarpal joint but require the accompaniment of the midcarpal joint and intercarpal joints (joints in between the carpal bones). Some movement is required between those bones, but movement becomes problematic.
Common Wrist Problems
Capitate Subluxation
The scaphoid and hamate bones are associated with fractures due to their location on effect nevertheless, the capitate bone is significantly more vulnerable to other athletic trauma, mostly subluxation, due to its substantial size, elongated silhouette using a narrower distal end, along with its central position, which makes it articulate with seven of those other carpal bones. These properties can encourage subluxation to occur with wrist trauma, Pressure to just laxity and instability or the joint around the bone.Carpal bone instability may be misdiagnosed, or even overlooked, but a capitate subluxation has a presentation that was typical. The individual clunking at the wrist joint on loading bearing exercises and usually does not have any history of trauma but complains of protracted weeks of pain. After exercise there is annoyance or an irregular niggle from the region of the capitate.
Wrist extension would be restricted and painful every time, whereas flexion wouldn’t be limited. Flexion can become debilitating over time since the ligaments become pulled on account of the subluxation causing them to stretch that is over. There may be a dip in the end and a bulge at one point where the bone has moved out from its groove that is carpal.
Solutions To Wrist Extension Problems
Rehabilitation of a wrist injury should firstly concentrate on reducing inflammation and pain so that therapy can proceed efficiently. This may involve the use of in ice and severe conditions, immobilization of the wrist to permit no strain and for the recovery process to begin. Range of motion should be increased where possible, and this might involve manual treatment (as described below) if there’s a physical block to motion. Progression then should concentrate on strengthening the weakened ligaments and muscles and restoring the wrist to sports specific conditioning, coordination and flexibility (5). A return to game ought to be executed and this may require the use of splints or grips originally to gauge the suitability of wrist recovery for your sport’s demands.1) Manual Therapy
If the capitate has subluxed then it ought to first be reduced (put back in position) by an experienced orthopedic physiotherapist. They will bend the wrist to relax the ligaments and also apply a surprising push whilst applying grip the distance. A palpable clunk will signify the decrease in the capitate and ordinary carpal alignment should then be felt (6). The athlete may feel an immediate relief of symptoms and once is sufficient to restore normal function and recover wrist extension. Based on the laxity of the carpal ligaments, subluxation may re-occur and the procedure should be repeated, as well as following the following steps for prevention.
2) Soft Tissue Stretching
Stretching of some of the upper limb since we discussed intricately linked fascia and the body’s connective tissues are muscles would be of benefit. One muscle will have consequences elsewhere. Particular care ought to be taken to the forearm flexors and extensors and these may be elongated holding for 30 minutes and by placing the wrist into extension or flexion.Global stretching for the upper limb can be performed utilizing the stretches pictured below.


3) The Use Of Hand Bars
Where flooring strength work is vital to training, like press-ups and boards, rather than force the wrist can utilize hand bars. This keeps the wrist in a neutral position and allows you to grasp the handle. This could be recommended for people who have a capitate subluxation also to prevent future injuries and to minimize the strain.4) Wrist Splints/Supports
For activities occur frequently, the use of a splint or support can decrease. This may be a viable option if the injury is secure and will not receive loading splinting isn’t the solution to unstable or severe injuries where certain treatment should be the priority over all instruction (3). The type of support will depend on the harm, your sport, and movement you need to continue looking for advice will be valuable here.5) Strengthening Exercises
Strengthening the surrounding muscles the wrist is needed to take care of but in addition to further absorb the shock to the wrist in effect and increase its own protection.Ball Squeezes — This can be made sports- Specific by using your own sports racquet, ball or similarly. Squeeze the object in your hands for five seconds and then release; replicating for 3 sets of 10. By holding the thing in exactly the positions you’d in game eg holding your tennis racquet at the position as well as in front of you this may be defined.
Wrist Flexion — Start by holding a little Weight on your hands with your arm down by your side and the palm facing you. Raise the hands upwards into wrist flexion and repeat for three sets of 10.
Wrist extension — Repeat the above possess the palms although description Body that increasing the back of the hand The wrist is brought by upwards into expansion.
References
1. Am J Sports Med. 2003; 31(6), 1038-1048.
2. Maitland’s Peripheral Manipulation (2014). 5th Ed. Vol II. Churchill Livingstone. Elsevier. pp 327.
3. Sports Health. 2009; 1(6), 469-477.
4. Anatomy Trains (2013). 3rd Ed. Churchill Livingstone. Elsevier.
5. Prim Care Clin Office Pract. 2005; 32, 35-70.
6. Curr Orthop Pract. 2012;23(4), 318-321.
