




Chiropractor, Dr. Alexander Jimenez examines the relevant anatomy and biomechanics of the tensor fascia latae. He explains, what role it plays in pain and dysfunction, and what can be done in the presence of a tight and overactive TFL muscle.
The tensor fascia latae (TFL) is a hip muscle that is well known to rehabilitation therapists and allied health practitioners. It is a muscle that may play a role in pain and dysfunction in the lower limb, pelvis and spine. It is however poorly understood, as the research studies that exist on this muscle are few and far between. Furthermore, much of the research and opinions have simplified the exact anatomy of, not only the TFL, but also its anatomical relationship to the iliotibial band (ITB).
TFL is a muscle that has a complex anatomical arrangement with the ITB, and it performs various functional roles – not only in producing hip movement, but also imparting fascial tension through the fascia latae of the thigh and the specialised ITB. Therefore TFL also plays a key role in not only postural support during one legged stance, but also in limiting the tensile stress on the femur caused by the combination of bodyweight, ground reaction force and how these create unique bending forces on the femur.
Regional Anatomy
Discussing the anatomy of the TFL cannot be done in isolation without also discussing the anatomy of the iliotibial band/tract (ITB or ITT). Pare et al (1981) have presented arguably the most comprehensive anatomical and electomyographical study (EMG) study on the TFL to date(1). This followed a much earlier study in 1958 when Kaplan presented an exhaustive study on the TFL and iliotibial tract(2).Interestingly, Kaplan extended his study further by comparing the TFL and ITB in humans to other primate and mammals and discovered that human beings are the only mammals to have a defined ITB. Gottschalk et al (1997) also added a substantial amount of knowledge regarding the anatomy and function of both the TFL and ITB(3). In this millennium, Fairclough et al (2006)(4) and Feto et al (2002)(5) have provided even further knowledge of the TFL and its relationship to the ITB via cadaveric and biomechanical modelling studies.
TFL & MLL
The general consensus is that the TFL originates on the iliac crest starting at the ASIS (just lateral to the origin of the sartorious), and extends posteriorly along the iliac crest about 2 to 5 cm to incorporate both bony investments into the iliac crest and investments onto the gluteal fascia(1-3). Pare et al (1981) highlights that the muscle actually has two functionally and anatomically distinct heads – the anteromedial (AM) and posterolateral (PM) head(1). These will be discussed in detail later.The contentious issue however, is where the muscle ultimately inserts. It appears from available research, that the muscle has both a bony insertion onto the femur and a fascial insertion onto the ITB – or more specifically onto the specialised portion of the middle longitudinal layer (MLL) of the fascia lata of the thigh which we know as the ITB (see figure 1).

The ITB, also called the ‘band of Maissiat’, was originally studied in 1843
and was perceived to be a ligament that connected the ilium with the knee and was responsible for maintaining the balance of the body in stance and in motion(5). Later work by Kaplan (1954)(2) showed that human beings are the only mammals to own a distinct facial lateral band down the thigh highlighting further that the ITB may play a role in bipedal stance and balance(2). This view was further supported in biomechanical models suggested by Feto et al (2002)(5).
However, much later cadaveric studies showed that the exact anatomy of the ITB and its relationship to the TFL and gluteals was in fact far more complex. The fascia lata of the thigh has a rather multifaceted array of layers that all interconnect. Of particular importance to the TFL, is the middle longitudinal layer (MLL) of the fascia lata. The MLL is a thick, longitudinal connective tissue, commencing on the iliac crest and extending downwards to have several insertions. A large portion of the MLL blends with the inner transverse layer of the fascia lata to insert directly onto the femur. The MLL also has superficial fibres that extend all the way down to insert about the knee.
Anteriorly at the hip, the MLL envelopes the TFL so that this muscle is effectively joined and sandwiched between the superficial and deep MLL. It also has fibres that directly blend with the superficial fibres of the gluteus maximus The MLL therefore is joined in part to the gluteus maximus, and in part to the TFL.
To make things even more complex, as well as being enveloped by the MLL, some of the distal fibres of both heads of the TFL then insert into the MLL. The anteromedial fibres of the TFL blend with the MLL and course down the thigh to insert onto the lateral patella retinaculum. Therefore, this may influence somewhat the patella position in relation to the femoral trochlear groove.
However, none of these anteromedial fibres cross the knee joint to insert onto Gerdy’s tubercle, therefore they have no effect on motion at the tibia; the primary role appears to be at the hip. Some of the fibres (not all) of the posterolateral TFL, along with those superficial fibres of the gluteus maximus, invest onto the MLL and insert all the way down onto the lateral tubercle of the tibia. They therefore do cross the knee joint and thus may have a role in a stabilising the pelvis and the lower limb.
Inner TFL
What needs to be pointed out about the MLL, is that as it courses down the thigh it blends quite heavily with the inner transverse layer of the fascia lata(4). The inner transverse layer is quite developed and dense in the upper third of the thigh. These transverse fibres run obliquely to anchor strongly to the femur(4). These transverse layers represent part of the fibres that constitute the deep, thick intermuscular septum of the femur. This septum effectively forms an osteo-fascial wall between the anterior quadriceps muscle group and the posterior hamstring muscle group.Fibres from the inner transverse layer also accept the superior fibres of the gluteus maximus to form an ascending tendon. The portion of the posterolateral TFL that did not blend with the MLL also blended with this ascending tendon to insert directly onto the intermuscular septum – and thus the femur. In other words, the majority of the TFL indirectly inserts onto the femur via the ascending gluteal tendon, and indirectly via the blending of the MLL to the thick transverse layer.
Further down the thigh, the ITB remains a thickened portion of the fascia lata, creating the fascial barrier between the anterior quadriceps and the posterior hamstrings. It completely surrounds the thigh, is anchored to the distal lateral femoral shaft by strong obliquely directed fibrous strands that can represent a tendon enthuses, and is continuous with the patellar retinaculum(4). The presence of these fibrous anchoring strands divides the ITB into a proximal ‘tendinous’ portion and a distal ‘ligamentous’ portion(4). Therefore Fairclough et al (2006) argue that the TFL has very little involvement in tibia movement and knee function and its role is primarily directed at the hip(4).
Based on the current anatomical understanding of the TFL, the following points can be summarised;
2. Femur via the ascending gluteal tendon
In pure open kinetic-chain movement, the AM fibres are most active in hip flexion movements and also in abduction movements. It is silent however if the hip is externally rotated whilst abducting – an important consideration when prescribing hip rehabilitation exercises for the gluteals and other hip external rotators(6).
Based on the current anatomical understanding of the TFL, the following points can be summarised;
- The anterolateral fibres of the TFL blend with a component of the MLL that inserts onto the lateral patella retinaculum.
- The posterolateral fibres insert into essentially 2 parts:
2. Femur via the ascending gluteal tendon
- The superficial MLL appears to course downwards to insert either onto the patella or the tibia.
- The deep MLL inserts onto the femur, via its thick blending with the deep transverse layer of the fascia latae.
Function Of The TFL
Anteromedial fibres (AM)
The main role of this functional head is to flex the hip in open kinetic chain movements such as hip flexion during the swing phase of gait. This has been confirmed via EMG and electrical stimulation experiments(1). The muscle becomes silent upon heel strike, suggesting that the muscle needs to be inactive to allow hip extension to occur during stance phase. The muscle is most active during the acceleration phase of running, again suggesting its main role is as a powerful hip flexor(1).In pure open kinetic-chain movement, the AM fibres are most active in hip flexion movements and also in abduction movements. It is silent however if the hip is externally rotated whilst abducting – an important consideration when prescribing hip rehabilitation exercises for the gluteals and other hip external rotators(6).
Posterolateral fibres (PL)
These fibres are most active during stance phase of gait. This suggests the muscle acts as a major hip stabiliser in single leg stance by activating its hip abduction role. Interestingly the superior portion of the gluteus maximus is also active during this walking phase. Considering that the PL head has fibres that join the tendon coming from the superior gluteus maximus, this suggests that the PL fibres and superior gluteus maximus work synergistically to control pelvic stability in stance phase(1).Both the TFL and gluteus maximus exert their influence as a hip muscle through the investments they have with the MLL, the deep transverse layer of the fascia lata and the intermuscular septum. They effectively insert onto the femur via this complex web of fascia and are thus considered muscles originating at the pelvis and inserting onto the femur. In pure open kinetic chain movements, the PL fibres are active in all hip internal rotation movements and in abduction movements. Similar to the AM fibres, the PL fibres stay silent if the hip is abducting whilst in external rotation(6).
Role At The knee
Most of the comprehensive studies investigating the role of TFL in influencing knee movements and patella stability find it difficult to identify a direct role for the TFL in knee function. It almost certainly does not contribute to knee extension, flexion or rotation(4). Therefore, all previous descriptions of the TFL being a synergistic knee extender with the quadriceps or an externally rotator of the tibia can almost certainly be discarded. It is also doubtful that the TFL plays an active role in pulling the patella laterally. The most likely role the TFL has in knee patella stability is indirectly, through maintaining the tension in the fascia lata and thus the distal portion of the ITB that blends with the patella retinaculum(10).The TFL As A ‘Fascial Tensioner’
It has been suggested that the TFL also acts on the fascia latae of the thigh by maintaining fascia tension during movement. Mike Benjamin in 2009 highlighted how extensive the fascia lata of the thigh is(7). It is a complex arrangement of fascial planes that have variable thickness and development over the thigh. It has a loose anterior and posterior layer, which cover the quadriceps and hamstrings respectively. The loose anterior superficial layer would most likely ‘bunch up’ during knee extension movements if there did not exist some manner of tensioning system for the fascia to maintain the fascial envelope. Similarly, the posterior fascia latae would most likely bunch up during knee flexion movements.The most likely muscles to maintain this fascial tension during knee movement, based on their anatomical arrangement with the fascia lata would be the TFL anteriorly and superior gluteus maximus posteriorly. That is, the TFL would become slightly active in knee extension to gradually retract the fascia upwards whilst the knee extended – to prevent crimping and buckling of the anterior fascia. Similarly, the gluteus maximus can maintain fascial tension during knee flexion movements.
Femur Tensile Force
One of the most fascinating roles assigned to the ITB is the role it has in reducing the bending and tensile force on the lateral femur. Humans walk on two feet, and for a part of the gait cycle they are in one-leg stance. This can create large lateral femur tensile forces and medial femur compression forces, which if left unchecked, would create a varus effect of the femur and effectively ‘bow’ the femur.In 1982, Jacob and Huggler (1982) investigated the function of the ITB and concluded that the varus bending forces on the femur could be partially relieved by tensioning the ITB(8). Even earlier than this, Rybicki et al (1972) looked at the stresses on the femur caused by the varus force on the bone and also found that by increasing the tension in the ITB the lateral tension force and the medial compression force on the femur would both be reduced(9). The attached musculature such as the TFL and gluteus maximus would further tension the ITB and reduce this lateral tension force on the femur.
Feto et al (2002) provide a comprehensive biomechanical review of the role that the ITB and associated muscles play on creating a ‘compression gradient’ along the lateral femur – effectively preventing distortion of the lateral femur due to the tensile effect of downwardly directed gravity on the varus forces acting on the femur(5).
TFL Dysfunction
For all the problems that the TFL poses to patients and therapists alike, almost nothing exists in the literature that highlights the role this muscle has in dysfunction. All theories and ideas are based on clinical reasoning and assumptions. The most interesting observation regarding TFL and dysfunction is the role it has in causing hip internal rotation/flexion during the stance phase of gait.It is common and habitual for patients complaining of lower limb overuse injuries or low back/SIJ pain to demonstrate an exaggerated hip flexion/ internal rotation position during functional movements on one leg. That is, they demonstrate a positive Trendelenberg sign during one-leg stance (opposite side of pelvis drops down) and the stance hip assumes an internally rotated and flexed position. It appears as if they are ‘dropping out the back pocket’ on their stance leg.
This pathomechanic then creates a valgus collapse at the knee joint, and this has a direct mechanical influence on the ‘Q angle’ of the knee. With an increase in the ‘Q angle’ the patella has a tendency to drag laterally and compress against the lateral femoral condyle. This may then lead to patellofemoral pain at the knee.
The most plausible explanation for the Trendelenburg sign and the valgus knee collapse is that the TFL maintains pelvic stability in one-leg stance by initiating its abduction role. However if unchecked, the TFL will also exhibit its hip flexion/internal rotation role. The gluteus maximus and other hip external rotators should in theory check this flexion/internal rotation by providing and equal and opposite external rotation/extension role.
Gottschalk et al (1989) highlighted how the gluteus medius and minimus primarily act on the hip joint by providing a compressive and stabilising role. They do little to assist in maintaining a stable pelvic position. This role is assigned to the TFL and gluteus maximus(3).
The underlying principle behind why the TFL is such an influential muscle in pelvic dysfunction, is that the TFL has the greatest mechanical advantage to influence the pelvis and hip joint. It is the most anterior muscle at the front of the hip. It therefore has the greatest leverage advantage to induce a flexion posture or an anterior tilt of the ilium. Viewing the hip from in front, the TFL is also the most lateral muscle on the hip. It also therefore has the greatest leverage to affect abduction of the hip. This explains why such as small muscle can have such a large influence.
Management
Assessing tightness in the TFL can be performed using an ‘Ober Test’ or a ‘Thomas Test’.Ober test (see figures 2a and 2b)
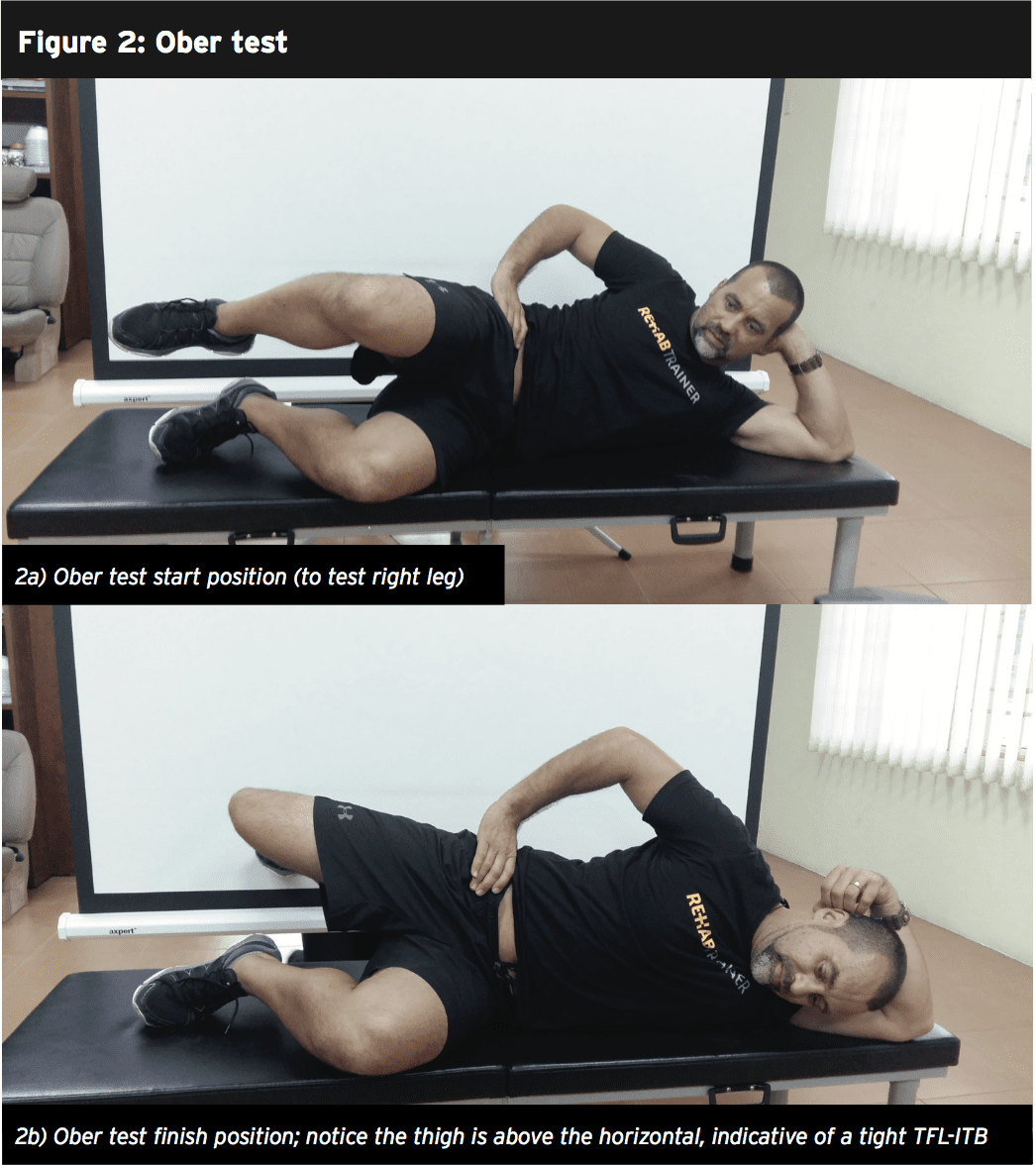
Start position – The client is positioned in side-lying, with the unaffected side down. The pelvis and spine are in neutral alignment, with the bottom leg flexed for support. The uppermost leg is extended and needs to be above the horizontal. The hip is laterally rotated and extended, as far as no lumbar extension occurs.
Movement – The client actively flattens the waist towards the floor and holds the leg in slight abduction and lateral rotation. He/she client is then instructed to slowly lower the leg towards the floor until the TFL-ITB hangs on the greater trochanter and cannot lower any further. The key to an accurate test is not letting the pelvis move, either into lateral tilt, anterior tilt or rotation. As the leg lowers, the hip should not flex or medially rotate. It’s essential to maintain the laterally rotated position of the hip. Ideally, the leg should lower into at least 10 to 15 degrees adduction without loss of proximal control of the pelvis or hip. The TFL-ITB lacks extensibility if the leg does not adduct sufficiently.
Thomas test (see figure 3)
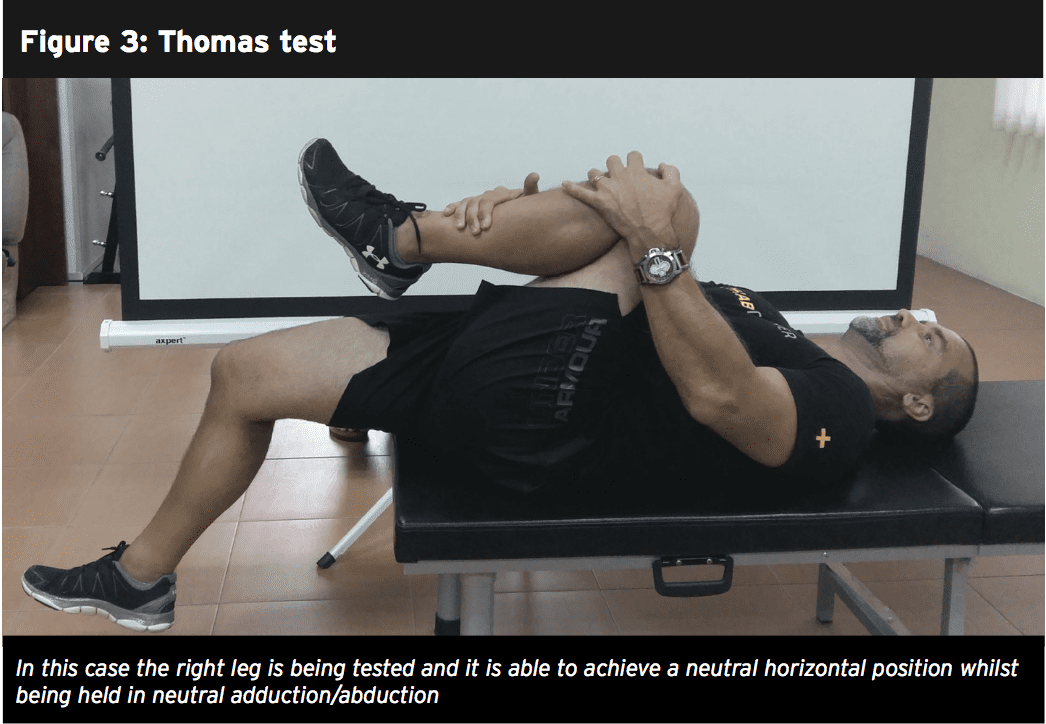
On a plinth, the patient lies supine, with the untested leg held in hip flexion. The tested leg is then forced into extension and adduction. If the tested leg is unable to attain a horizontal alignment and is held in flexion and/or abduction, this is indicative of tightness in the TFL.
Managing Tightness In The TFL
Managing the overactive/tight TFL comes with 2 important criteria: it must be stretched and it must be massaged/ manipulated. The most effective stretch for the TFL is in the knee-down hip flexor stretch (see figure 4). If you are stretching the left TFL: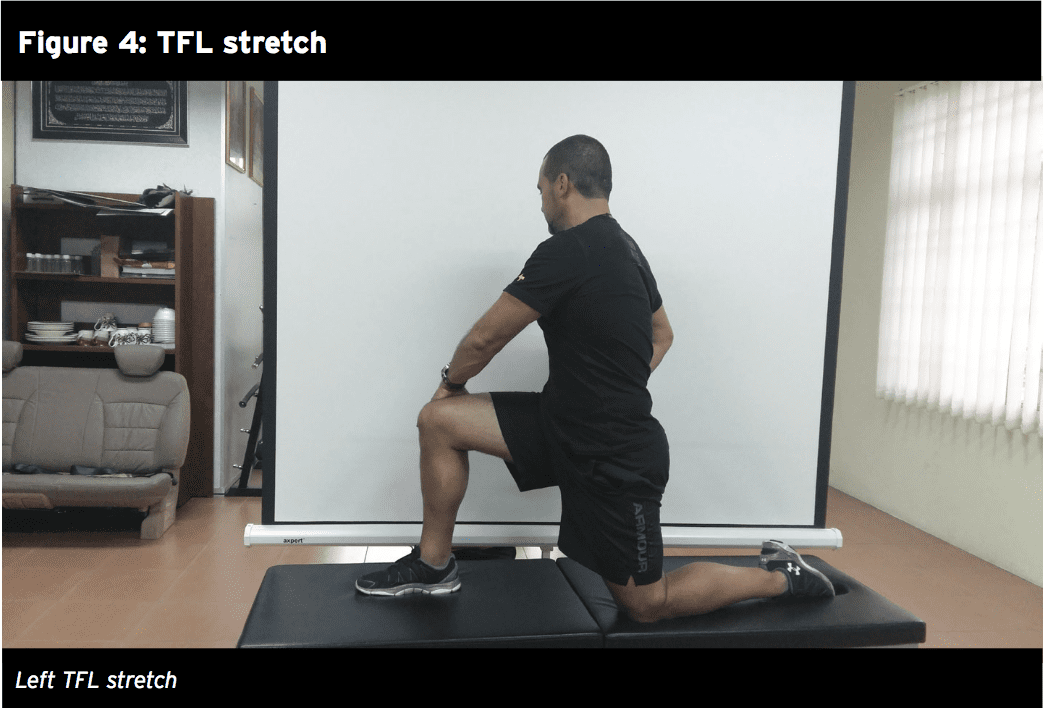
1. Kneel on the left knee with the right leg at 90 degrees hip flexion and knee flexion.
2. Push the left hip forward until the slack is taken up (this takes up the flexion component).
3. Place your hands on the right thigh and twist the trunk around to the right whilst the pelvis remains facing forward (this induces an external rotation of the hip which adds to the rotation component of the stretch).
4. If you have any slack left, push the left outwards (this takes up the abduction component).
5. Finally, isometrically contract the right hamstring by attempting to drag the left heel backwards (this induces posterior pelvis tilt that takes up the anterior tilt component).
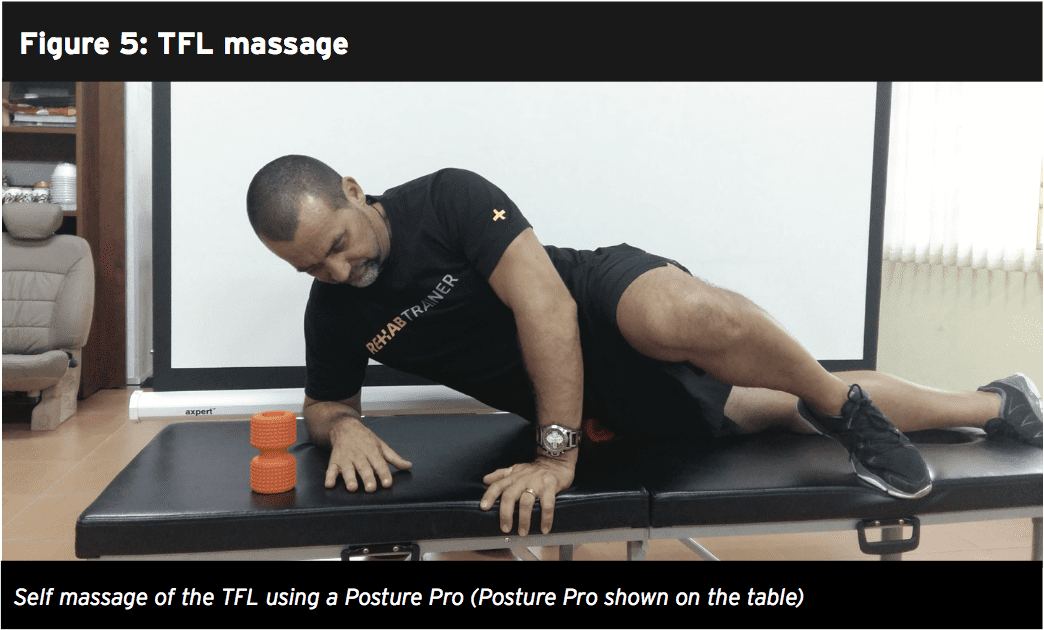
To self massage or trigger the TFL (figure 5), have the client lie on their side and place a trigger ball/Muscle Mate/Posture Pro under the TFL and apply gentle pressure. The hip, knee and ankle need to stay in a straight line with the body. This can be performed as a rolling type movement or as sustained pressure to relieve the trigger points within the muscle.
Conclusion
TFL is a muscle that acts both on the hip joint to create hip/pelvic dysfunction and it also acts on creating tension in the fascia latae and its specialised portion known as the ITB. Overactivity in this muscle can create a direct mechanical effect that creates excessive lateral tension on the patella and thus patellofemoral pain and it can also be implicated in low back syndromes that are caused by excessive anterior pelvic tilt and lumbar spine extension. It is a muscle that needs regular massage and stretching.References
1. Journal of Bone and Joint Surgery. 1981. 63: 1457-1471
2. Journal of Bone and Joint Surgery. 1958. 40: 817-832
3. Journal of Anatomy. 1989. 166: 179-189
4. J of Anatomy. 2006. 208; 309-316
5. J Orthop Sci. 2002. 7:724–730
6. Journal of orthopaedic & sports physical therapy. 2013. 43(2); 54-65
7. Journal of Anatomy. 2009. 214: 1-18
8. Jacob HA, Huggler AH. In vivo investigations of the mechanical function of the tractus iliotibialis. In Huiskes R, von Campen DH, de Wijn JR, editors. Biomechanics, principles and applications: selected proceedings of the 3rd General Meeting of the European Society of Biomechanics, Nijmegen, The Netherlands, January 1982. The Hague: Nijhoff; 1982
9. J Biomech. 1972;5:203–15
10. Journal of Arthroscopic and Related Research. 2007. 23(3): 269-274
