




The knee is one of the most complex joints in the human body, consisting of the thigh bone, or femur, the shin bone, or tibia, and the kneecap, or patella, among other soft tissues. Tendons connect the bones to the muscles while ligaments connect the bones of the knee joint. Two wedge-shaped pieces of cartilage, known as the meniscus, provide stability to the knee joint. The purpose of the article below is to demonstrate as well as discuss the anatomy of the knee joint and its surrounding soft tissues.
Abstract
- Context: Information regarding the structure, composition, and function of the knee menisci has been scattered across multiple sources and fields. This review contains a concise, detailed description of the knee menisci—including anatomy, etymology, phylogeny, ultrastructure and biochemistry, vascular anatomy and neuroanatomy, biomechanical function, maturation and aging, and imaging modalities.
- Evidence Acquisition: A literature search was performed by a review of PubMed and OVID articles published from 1858 to 2011.
- Results: This study highlights the structural, compositional, and functional characteristics of the menisci, which may be relevant to clinical presentations, diagnosis, and surgical repairs.
- Conclusions: An understanding of the normal anatomy and biomechanics of the menisci is a necessary prerequisite to understanding the pathogenesis of disorders involving the knee.
- Keywords: knee, meniscus, anatomy, function
Introduction
Once described as a functionless embryonic remnant,162 the menisci are now known to be vital for the normal function and long-term health of the knee joint.§ The menisci increase stability for femorotibial articulation, distribute axial load, absorb shock, and provide lubrication and nutrition to the knee joint.4,91,152,153
Injuries to the menisci are recognized as a cause of significant musculoskeletal morbidity. The unique and complex structure of menisci makes treatment and repair challenging for the patient, surgeon, and physical therapist. Furthermore, long-term damage may lead to degenerative joint changes such as osteophyte formation, articular cartilage degeneration, joint space narrowing, and symptomatic osteoarthritis.36,45,92 Preservation of the menisci depends on maintaining their distinctive composition and organization.
Anatomy of Menisci
Meniscal Etymology
The word meniscus comes from the Greek word mēniskos, meaning “crescent,” diminutive of mēnē, meaning “moon.”
Meniscal Phylogeny and Comparative Anatomy
Hominids exhibit similar anatomic and functional characteristics, including a bicondylar distal femur, intra-articular cruciate ligaments, menisci, and asymmetrical collateral.40,66 These similar morphologic characteristics reflect a shared genetic lineage that can be traced back more than 300 million years.40,66,119
In the primate lineage leading to humans, hominids evolved to bipedal stance approximately 3 to 4 million years ago, and by 1.3 million years ago, the modern patellofemoral joint was established (with a longer lateral patellar facet and matching lateral femoral trochlea).164 Tardieu investigated the transition from occasional bipedalism to permanent bipedalism and observed that primates contain a medial and lateral fibrocartilaginous meniscus, with the medial meniscus being morphologically similar in all primates (crescent shaped with 2 tibial insertions).163 By contrast, the lateral meniscus was observed to be more variable in shape. Unique in Homo sapiens is the presence of 2 tibial insertions—1 anterior and 1 posterior—indicating a habitual practice of full extension movements of the knee joint during the stance and swing phases of bipedal walking.20,134,142,163,168
Embryology and Development
The characteristic shape of the lateral and medial menisci is attained between the 8th and 10th week of gestation.53,60 They arise from a condensation of the intermediate layer of mesenchymal tissue to form attachments to the surrounding joint capsule.31,87,110 The developing menisci are highly cellular and vascular, with the blood supply entering from the periphery and extending through the entire width of the menisci.31 As the fetus continues to develop, there is a gradual decrease in the cellularity of the menisci with a concomitant increase in the collagen content in a circumferential arrangement.30,31 Joint motion and the postnatal stress of weightbearing are important factors in determining the orientation of collagen fibers. By adulthood, only the peripheral 10% to 30% have a blood supply.12,31
Despite these histologic changes, the proportion of tibial plateau covered by the corresponding meniscus is relatively constant throughout fetal development, with the medial and lateral menisci covering approximately 60% and 80% of the surface areas, respectively.31
Gross Anatomy
Gross examination of the knee menisci reveals a smooth, lubricated tissue (Figure 1). They are crescent-shaped wedges of fibrocartilage located on the medial and lateral aspects of the knee joint (Figure 2A). The peripheral, vascular border (also known as the red zone) of each meniscus is thick, convex, and attached to the joint capsule. The innermost border (also known as the white zone) tapers to a thin free edge. The superior surfaces of menisci are concave, enabling effective articulation with their respective convex femoral condyles. The inferior surfaces are flat to accommodate the tibial plateau (Figure 1).28,175
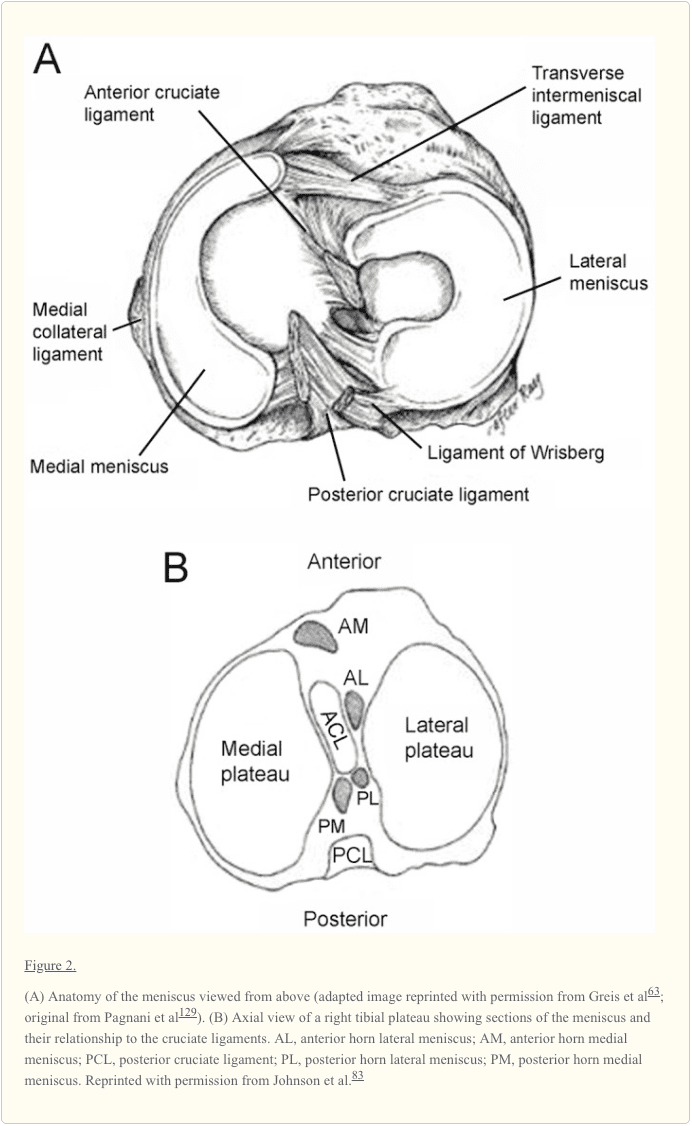
The tibial portion of the capsular attachment is the coronary ligament. At its midpoint, the medial meniscus is more firmly attached to the femur through a condensation in the joint capsule known as the deep medial collateral ligament.175 The transverse, or “intermeniscal,” ligament is a fibrous band of tissue that connects the anterior horn of the medial meniscus to the anterior horn of the lateral meniscus (Figures 1 and and2A2A).
Lateral meniscus. The lateral meniscus is almost circular, with an approximately uniform width from anterior to posterior (Figures 1 and and2A).2A). It occupies a larger portion (~80%) of the articular surface than the medial meniscus (~60%) and is more mobile.10,31,165 Both horns of the lateral meniscus are attached to the tibia. The insertion of the anterior horn of the lateral meniscus lies anterior to the intercondylar eminence and adjacent to the broad attachment site of the ACL (Figure 2B).9,83 The posterior horn of the lateral meniscus inserts posterior to the lateral tibial spine and just anterior to the insertion of the posterior horn of the medial meniscus (Figure 2B).83 The lateral meniscus is loosely attached to the capsular ligament; however, these fibers do not attach to the lateral collateral ligament. The posterior horn of the lateral meniscus attaches to the inner aspect of the medial femoral condyle via the anterior and posterior meniscofemoral ligaments of Humphrey and Wrisberg, respectively, which originate near the origin of the PCL (Figures 1 and and22).75
Meniscofemoral ligaments. The literature reports significant inconsistencies in the presence and size of meniscofemoral ligaments of the lateral meniscus. There may be none, 1, 2, or 4.‖ When present, these accessory ligaments transverse from the posterior horn of the lateral meniscus to the lateral aspect of the medial femoral condyle. They insert immediately adjacent to the femoral attachment of the PCL (Figures 1 and and22).
In a series of studies, Harner et al measured the cross-sectional area of the ligaments and found that the meniscofemoral ligament averaged 20% of the size of the PCL (range, 7%-35%).69,70 However, the size of the insertional area alone without knowledge of the insertional angle or collagen density does not indicate their relative strength.115 The function of these ligaments remains unknown; they may pull the posterior horn of the lateral meniscus in an anterior direction to increase the congruity of the meniscotibial fossa and the lateral femoral condyle.75
Ultrastructure and Biochemistry
Extracellular Matrix
The meniscus is a dense extracellular matrix (ECM) composed primarily of water (72%) and collagen (22%), interposed with cells.9,55,56,77 Proteoglycans, noncollagenous proteins, and glycoproteins account for the remaining dry weight.¶ Meniscal cells synthesize and maintain the ECM, which determines the material properties of the tissue.
The cells of the menisci are referred to as fibrochondrocytes because they appear to be a mixture of fibroblasts and chondrocytes.111,177 The cells in the more superficial layer of the menisci are fusiform or spindle shaped (more fibroblastic), whereas the cells located deeper in the meniscus are ovoid or polygonal (more chondrocytic).55,56,178 Cell morphology does not differ between the peripheral and central locations in the menisci.56
Both cell types contain abundant endoplasmic reticulum and Golgi complex. Mitochondria are only occasionally visualized, suggesting that the major pathway for energy production of fibrochondrocytes in their avascular milieu is probably anaerobic glycolysis.112
Water
In normal, healthy menisci, tissue fluid represents 65% to 70% of the total weight. Most of the water is retained within the tissue in the solvent domains of proteoglycans. The water content of meniscal tissue is higher in the posterior areas than in the central or anterior areas; tissue samples from surface and deeper layers had similar contents.135
Large hydraulic pressures are required to overcome the drag of frictional resistance of forcing fluid flow through meniscal tissue. Thus, interactions between water and the matrix macromolecular framework significantly influence the viscoelastic properties of the tissue.
Collagens
Collagens are primarily responsible for the tensile strength of menisci; they contribute up to 75% of the dry weight of the ECM.77 The ECM is composed primarily of type I collagen (90% dry weight) with variable amounts of types II, III, V, and VI.43,44,80,112,181 The predominance of type I collagen distinguishes the fibrocartilage of menisci from articular (hyaline) cartilage. The collagens are heavily cross-linked by hydroxylpyridinium aldehydes.44
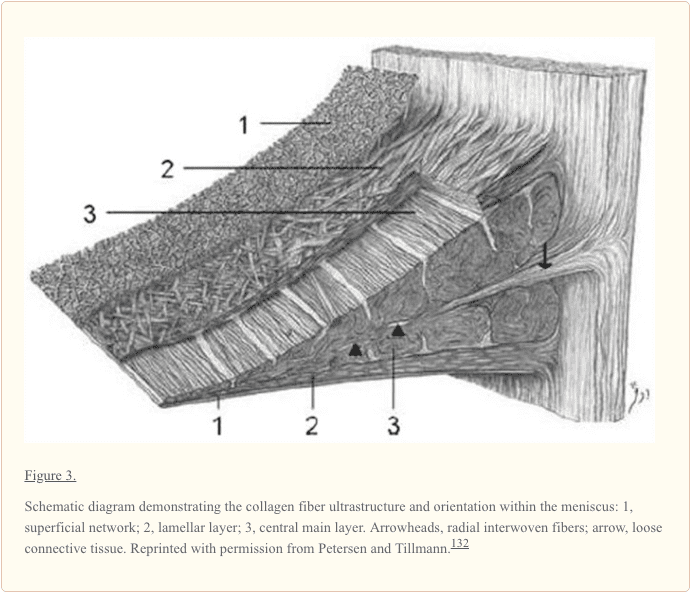
The collagen fiber arrangement is ideal for transferring a vertical compressive load into circumferential “hoop” stresses (Figure 3).57 Type I collagen fibers are oriented circumferentially in the deeper layers of the meniscus, parallel to the peripheral border. These fibers blend the ligamentous connections of the meniscal horns to the tibial articular surface (Figure 3).10,27,49,156 In the most superficial region of the menisci, the type I fibers are oriented in a more radial direction. Radially oriented “tie” fibers are also present in the deep zone and are interspersed or woven between the circumferential fibers to provide structural integrity (Figure 3).# There is lipid debris and calcified bodies in the ECM of human menisci.54 The calcified bodies contain long, slender crystals of phosphorous, calcium, and magnesium on electron-probe roentgenographic analysis.54 The function of these crystals in not completely understood, but it is believed that they may play a role in acute joint inflammation and destructive arthropathies.
Proteoglycans
Located within a fine meshwork of collagen fibrils, proteoglycans are large, negatively charged hydrophilic molecules, contributing 1% to 2% of dry weight.58 They are formed by a core protein with 1 or more covalently attached glycosaminoglycan chains (Figure 4).122 The size of these molecules is further increased by specific interaction with hyaluronic acid.67,72 The amount of proteoglycans in the meniscus is one-eighth that of articular cartilage,2,3 and there may be considerable variation depending on the site of the sample and the age of the patient.49
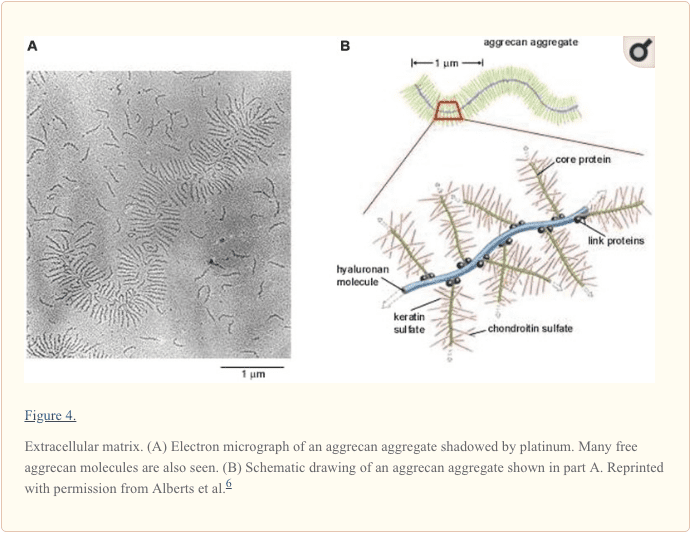
Aggrecan is the major proteoglycan found in the human menisci and is largely responsible for their viscoelastic compressive properties (Figure 5). Smaller proteoglycans, such as decorin, biglycan, and fibromodulin, are found in smaller amounts.124,151 Hexosamine contributes 1% to the dry weight of ECM.57,74 The precise functions of each of these small proteoglycans on the meniscus have yet to be fully elucidated.
Matrix Glycoproteins
Meniscal cartilage contains a range of matrix glycoproteins, the identities and functions of which have yet to be determined. Electrophoresis and subsequent staining of the polyacrylamide gels reveals bands with molecular weights varying from a few kilodaltons to more than 200 kDa.112 These matrix molecules include the link proteins that stabilize proteoglycan–hyaluronic acid aggregates and a 116-kDa protein of unknown function.46 This protein resides in the matrix in the form of disulfide-bonded complex of high molecular weight.46 Immunolocalization studies suggest that it is predominantly located around the collagen bundles in the interterritorial matrix.47
The adhesive glycoproteins constitute a subgroup of the matrix glycoproteins. These macromolecules are partly responsible for binding with other matrix molecules and/or cells. Such intermolecular adhesion molecules are therefore important components in the supramolecular organization of the extracellular molecules of the meniscus.150 Three molecules have been identified within the meniscus: type VI collagen, fibronectin, and thrombospondin.112,118,181
Vascular Anatomy
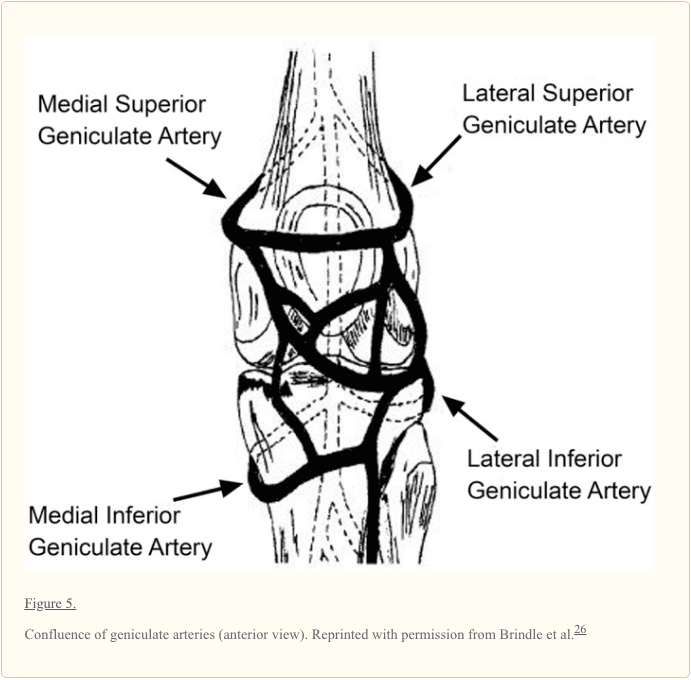
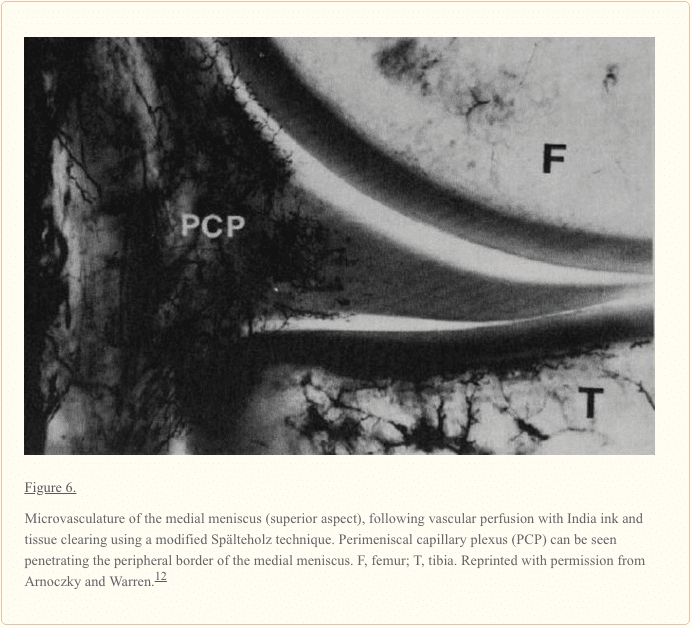
The meniscus is a relatively avascular structure with a limited peripheral blood supply. The medial, lateral, and middle geniculate arteries (which branch off the popliteal artery) provide the major vascularization to the inferior and superior aspects of each meniscus (Figure 5).9,12,33-35,148 The middle geniculate artery is a small posterior branch that perforates the oblique popliteal ligament at the posteromedial corner of the tibiofemoral joint. A premeniscal capillary network arising from the branches of these arteries originates within the synovial and capsular tissues of the knee along the periphery of the menisci. The peripheral 10% to 30% of the medial meniscus border and 10% to 25% of the lateral meniscus are relatively well vascularized, which has important implications for meniscus healing (Figure 6).12,33,68 Endoligamentous vessels from the anterior and posterior horns travel a short distance into the substance of the menisci and form terminal loops, providing a direct route for nourishment.33 The remaining portion of each meniscus (65% to 75%) receives nourishment from synovial fluid via diffusion or mechanical pumping (ie, joint motion).116,120
Neuroanatomy
The knee joint is innervated by the posterior articular branch of the posterior tibial nerve and the terminal branches of the obturator and femoral nerves. The lateral portion of the capsule is innervated by the recurrent peroneal branch of the common peroneal nerve. These nerve fibers penetrate the capsule and follow the vascular supply to the peripheral portion of the menisci and the anterior and posterior horns, where most of the nerve fibers are concentrated.52,90 The outer third of the body of the meniscus is more densely innervated than the middle third.183,184 During extremes of flexion and extension of the knee, the meniscal horns are stressed, and the afferent input is likely greatest at these extreme positions.183,184
The mechanoreceptors within the menisci function as transducers, converting the physical stimulus of tension and compression into a specific electrical nerve impulse. Studies of human menisci have identified 3 morphologically distinct mechanoreceptors: Ruffini endings, Pacinian corpuscles, and Golgi tendon organs.‡‡ Type I (Ruffini) mechanoreceptors are low threshold and slowly adapting to the changes in joint deformation and pressure. Type II (Pacinian) mechanoreceptors are low threshold and fast adapting to tension changes.§§ Type III (Golgi) are high-threshold mechanoreceptors, which signal when the knee joint approaches the terminal range of motion and are associated with neuromuscular inhibition. These neural elements were found in greater concentration in the meniscal horns, particularly the posterior horn.
The asymmetrical components of the knee act in concert as a type of biological transmission that accepts, transfers, and dissipates loads along the femur, tibia, patella, and femur.41 Ligaments act as an adaptive linkage, with the menisci representing mobile bearings. Several studies have reported that various intra-articular components of the knee are sensate, capable of generating neurosensory signals that reach spinal, cerebellar, and higher central nervous system levels.‖‖ It is believed that these neurosensory signals result in conscious perception and are important for normal knee joint function and maintenance of tissue homeostasis.42

The meniscus is cartilage which provides structural and functional integrity to the knee. The menisci are two pads of fibrocartilaginous tissue which spread out friction in the knee joint when it undergoes tension and torsion between the shin bone, or tibia, and the thigh bone, or femur. The understanding of the anatomy and biomechanics of the knee joint is essential towards the understanding of knee injuries and/or conditions. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Biomechanical Function
The biomechanical function of the meniscus is a reflection of the gross and ultrastructural anatomy and of its relationship to the surrounding intra-articular and extra-articular structures. The menisci serve many important biomechanical functions. They contribute to load transmission,¶¶ shock absorption,10,49,94,96,170 stability,51,100,101,109,155 nutrition,23,24,84,141 joint lubrication,102-104,141 and proprioception.5,15,81,88,115,147 They also serve to decrease contact stresses and increase contact area and congruity of the knee.91,172
Meniscal Kinematics
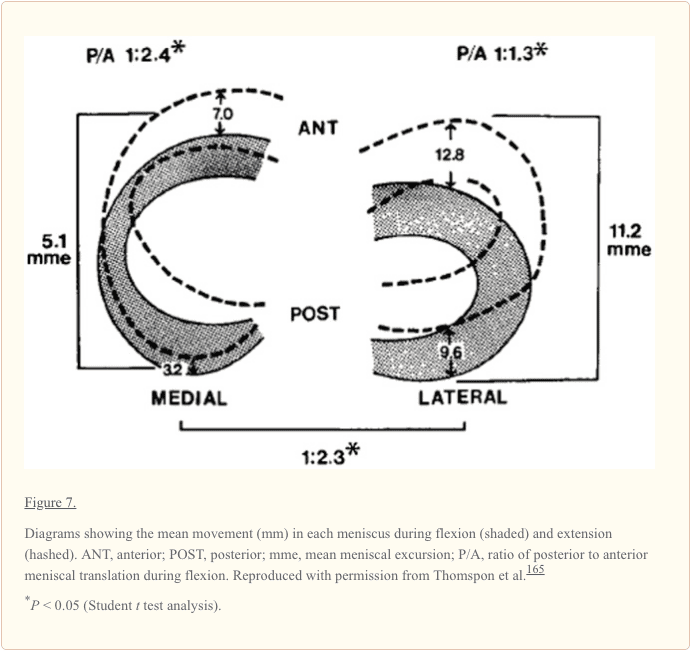
In a study on ligamentous function, Brantigan and Voshell reported the medial meniscus to move an average 2 mm, while the lateral meniscus was markedly more mobile with approximately 10 mm of anterior-posterior displacement during flexion.25 Similarly, DePalma reported that the medial meniscus undergoes 3 mm of anterior-posterior displacement, while the lateral meniscus moves 9 mm during flexion.37 In a study using 5 cadaveric knees, Thompson et al reported the mean medial excursion to be 5.1 mm (average of anterior and posterior horns) and the mean lateral excursion, 11.2 mm, along the tibial articular surface (Figure 7).165 The findings from these studies confirm a significant difference in segmental motion between the medial and lateral menisci. The anterior and posterior horn lateral meniscus ratio is smaller and indicates that the meniscus moves more as a single unit.165 Alternatively, the medial meniscus (as a whole) moves less than the lateral meniscus, displaying a greater anterior to posterior horn differential excursion. Thompson et al found that the area of least meniscal motion is the posterior medial corner, where the meniscus is constrained by its attachment to the tibial plateau by the meniscotibial portion of the posterior oblique ligament, which has been reported to be more prone to injury.143,165 A reduction in the motion of the posterior horn of the medial meniscus is a potential mechanism for meniscal tears, with a resultant “trapping” of the fibrocartilage between the femoral condyle and the tibial plateau during full flexion. The greater differential between anterior and posterior horn excursion may place the medial meniscus at a greater risk of injury.165
Load Transmission
The function of the menisci has been clinically inferred by the degenerative changes that accompany its removal. Fairbank described the increased incidence and predictable degenerative changes of the articular surfaces in completely meniscectomized knees.45 Since this early work, numerous studies have confirmed these findings and have further established the important role of the meniscus as a protective, load-bearing structure.
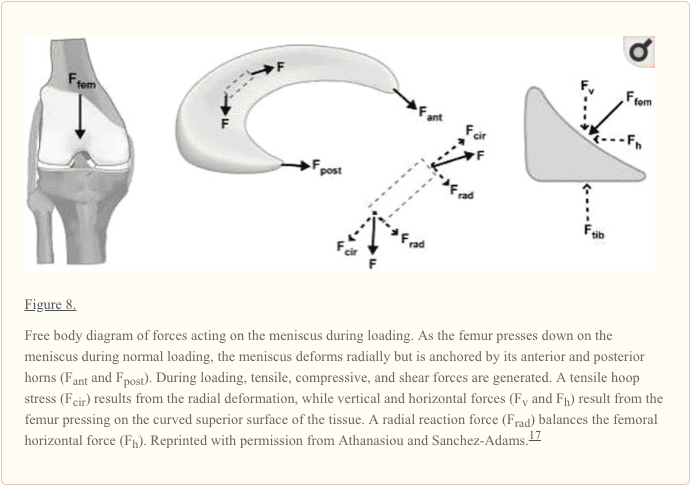
Weightbearing produces axial forces across the knee, which compress the menisci, resulting in “hoop” (circumferential) stresses.170 Hoop stresses are generated as axial forces and converted to tensile stresses along the circumferential collagen fibers of the meniscus (Figure 8). Firm attachments by the anterior and posterior insertional ligaments prevent the meniscus from extruding peripherally during load bearing.94 Studies by Seedhom and Hargreaves reported that 70% of the load in the lateral compartment and 50% of the load in the medial compartment is transmitted through the menisci.153 The menisci transmit 50% of compressive load through the posterior horns in extension, with 85% transmission at 90° flexion.172 Radin et al demonstrated that these loads are well distributed when the menisci are intact.137 However, removal of the medial meniscus results in a 50% to 70% reduction in femoral condyle contact area and a 100% increase in contact stress.4,50,91 Total lateral meniscectomy results in a 40% to 50% decrease in contact area and increases contact stress in the lateral component to 200% to 300% of normal.18,50,76,91 This significantly increases the load per unit area and may contribute to accelerated articular cartilage damage and degeneration.45,85
Shock Absorption
The menisci play a vital role in attenuating the intermittent shock waves generated by impulse loading of the knee with normal gait.94,96,153 Voloshin and Wosk showed that the normal knee has a shock-absorbing capacity about 20% higher than knees that have undergone meniscectomy.170 As the inability of a joint system to absorb shock has been implicated in the development of osteoarthritis, the meniscus would appear to play an important role in maintaining the health of the knee joint.138
Joint Stability
The geometric structure of the menisci provides an important role in maintaining joint congruity and stability.## The superior surface of each meniscus is concave, enabling effective articulation between the convex femoral condyles and flat tibial plateau. When the meniscus is intact, axial loading of the knee has a multidirectional stabilizing function, limiting excess motion in all directions.9
Markolf and colleagues have addressed the effect of meniscectomy on anterior-posterior and rotational knee laxity. Medial meniscectomy in the ACL-intact knee has little effect on anterior-posterior motion, but in the ACL-deficient knee, it results in an increase in anterior-posterior tibial translation of up to 58% at 90o of flexion.109 Shoemaker and Markolf demonstrated that the posterior horn of the medial meniscus is the most important structure resisting an anterior tibial force in the ACL-deficient knee.155 Allen et al showed that the resultant force in the medial meniscus of the ACL-deficient knee increased by 52% in full extension and by 197% at 60° of flexion under a 134-N anterior tibial load.7 The large changes in kinematics due to medial meniscectomy in the ACL-deficient knee confirm the important role of the medial meniscus in knee stability. Recently, Musahl et al reported that the lateral meniscus plays a role in anterior tibial translation during the pivot-shift maneuver.123
Joint Nutrition and Lubrication
The menisci may also play a role in the nutrition and lubrication of the knee joint. The mechanics of this lubrication remains unknown; the menisci may compress synovial fluid into the articular cartilage, which reduces frictional forces during weightbearing.13
There is a system of microcanals within the meniscus located close to the blood vessels, which communicates with the synovial cavity; these may provide fluid transport for nutrition and joint lubrication.23,24
Proprioception
The perception of joint motion and position (proprioception) is mediated by mechanoreceptors that transduce mechanical deformation into electric neural signals. Mechanoreceptors have been identified in the anterior and posterior horns of the menisci.*** Quick-adapting mechanoreceptors, such as Pacinian corpuscles, are thought to mediate the sensation of joint motion, and slow-adapting receptors, such as Ruffini endings and Golgi tendon organs, are believed to mediate the sensation of joint position.140 The identification of these neural elements (located mostly in the middle and outer third of the meniscus) indicates that the menisci are capable of detecting proprioceptive information in the knee joint, thus playing an important afferent role in the sensory feedback mechanism of the knee.61,88,90,158,169
Maturation and Aging of The Meniscus
The microanatomy of the meniscus is complex and certainly demonstrates senescent changes. With advancing age, the meniscus becomes stiffer, loses elasticity, and becomes yellow.78,95 Microscopically, there is a gradual loss of cellular elements with empty spaces and an increase in fibrous tissue in comparison with elastic tissue.74 These cystic areas can initiate a tear, and with a torsional force by the femoral condyle, the superficial layers of the meniscus may shear off from the deep layer at the interface of the cystic degenerative change, producing a horizontal cleavage tear. Shear between these layers may cause pain. The torn meniscus may directly injure the overlying articular cartilage.74,95
Ghosh and Taylor found that collagen concentration increased from birth to 30 years and remained constant until 80 years of age, after which a decline occurred.58 The noncollagenous matrix proteins showed the most profound changes, decreasing from 21.9% ± 1.0% (dry weight) in neonates to 8.1% ± 0.8% between the ages of 30 to 70 years.80 After 70 years of age, the noncollagenous matrix protein levels increased to 11.6% ± 1.3%. Peters and Smillie observed an increase in hexosamine and uronic acid with age.131
McNicol and Roughley studied the variation of meniscal proteoglycans in aging113; small differences in extractability and hydrodynamic size were observed. The proportions of keratin sulfate relative to chondroitin-6-sulfate increased with aging.146
Petersen and Tillmann immunohistochemically investigated human menisci (ranging from 22 weeks of gestation to 80 years), observing the differentiation of blood vessels and lymphatics in 20 human cadavers. At the time of birth, nearly the entire meniscus was vascularized. In the second year of life, an avascular area developed in the inner circumference. In the second decade, blood vessels were present in the peripheral third. After 50 years of age, only the peripheral quarter of the meniscal base was vascularized. The dense connective tissue of the insertion was vascularized but not the fibrocartilage of the insertion. Blood vessels were accompanied by lymphatics in all areas.†††
Arnoczky suggested that body weight and knee joint motion may eliminate blood vessels in the inner and middle aspects of the menisci.9 Nutrition of meniscal tissue occurs via perfusion from blood vessels and via diffusion from synovial fluid. A requirement for nutrition via diffusion is the intermittent loading and release on the articular surfaces, stressed by body weight and muscle forces.130 The mechanism is comparable with the nutrition of articular cartilage.22
Magnetic Resonance Imaging of The Meniscus
Magnetic resonance imaging (MRI) is a noninvasive diagnostic tool used in the evaluation, diagnosis, and monitoring of the menisci. MRI is widely accepted as the optimal imaging modality because of superior soft tissue contrast.
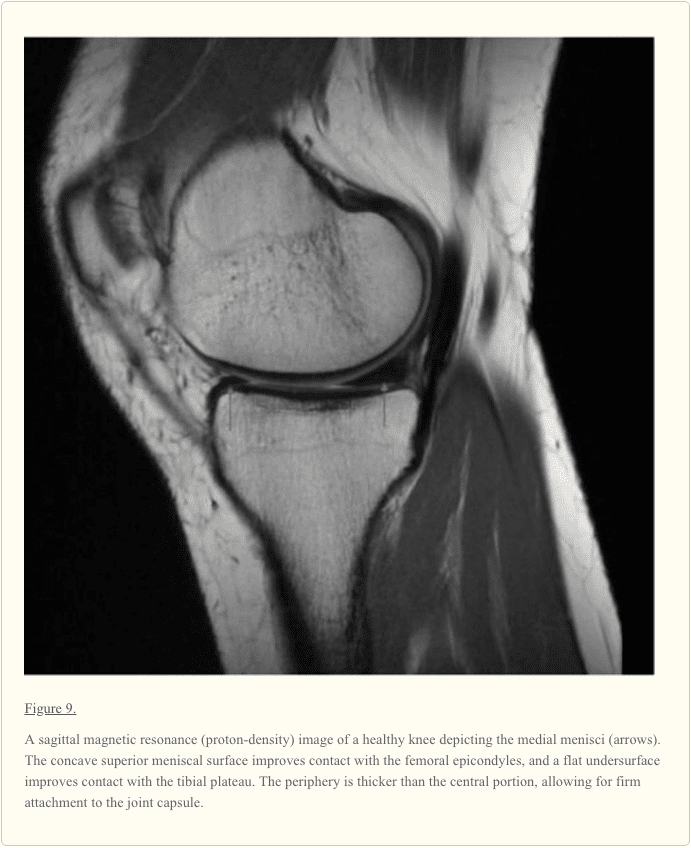
On cross-sectional MRI, the normal meniscus appears as a uniform low-signal (dark) triangular structure (Figure 9). A meniscal tear is identified by the presence of an increased intrameniscal signal that extends to the surface of this structure.
There have been discrepancies between MRI diagnoses and the pathology identified during arthroscopic examination.‡‡‡ Justice and Quinn reported discrepancies in the diagnosis of 66 of the 561 patients (12%).86 In a study of 92 patients, discrepancies between the MRI and arthroscopic diagnoses were noted in 22 of the 349 (6%) cases.106 Miller conducted a single-blind prospective study comparing clinical examinations and MRI in 57 knee examinations.117 He found no significant difference in sensitivity between the clinical examination and MRI (80.7% and 73.7%, respectively). Shepard et al assessed the accuracy of MRI in detecting clinically significant lesions of the anterior horn of the meniscus in 947 consecutive knee MRI154 and found a 74% false-positive rate. Increased signal intensity in the anterior horn does not necessarily indicate a clinically significant lesion.154
Conclusions
The menisci of the knee joint are crescent-shaped wedges of fibrocartilage that provide increased stability to the femorotibial articulation, distribute axial load, absorb shock, and provide lubrication to the knee joint. Injuries to the menisci are recognized as a cause of significant musculoskeletal morbidity. Preservation of the menisci is highly dependent on maintaining its distinctive composition and organization.
Acknowledgements
Ncbi.nlm.nih.gov/pmc/articles/PMC3435920/
Footnotes
Ncbi.nlm.nih.gov/pmc/articles/PMC3435920/
In conclusion, the knee is the largest and most complex joint in the human body. However, because the knee can commonly become damaged as a result of an injury and/or condition, it's essential to understand the anatomy of the knee joint in order for patients to receive proper treatment. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Referenced from: Ncbi.nlm.nih.gov

Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper's knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.

