




Bone Neoplasms Tumor-Like Conditions
- Bone neoplasms and tumor-like conditions affecting the knee can be benign or malignant. Age at Dx is crucial for DDx
- In patients <40: Benign bone neoplasms: Osteochondroma, Enchondroma are relatively frequent
- Fibrous cortical defect (FCD) & Non-ossifying fibroma (NOF) are particularly frequent in children
- Giant cell tumor (GCT) is the m/c benign neoplasm of the knee in patients between 20-40 years of age
- Malignant bone neoplasms in <40: m/c Osteosarcoma and 2nd m/c Ewing sarcoma
- In patients >40: malignant neoplasms: m/c are secondaries d/t bone metastasis. Primary bone malignancy: the m/c
- Multiple Myeloma (MM). Less frequently: a 2nd peak of Osteosarcoma (post-radiation or Paget’s), Fibrosarcoma or Malignant Fibrous Histiocytoma (MFH) of bone.
- Clinically: knee pain, pathological fracture
- Some tumor-like conditions like FCD/Non-ossifying fibroma are asymptomatic and may regress spontaneously.
Occasionally NOF may present with pathologic fracture. N.B. any knee/bone pain in a child/adolescents should be treated with clinical suspicion and adequately investigated. - Imaging: 1st step: radiography
- MRI with T1+C is crucial for lesion characterization/regional extent, staging and pre-operative planning. CT may help with pathologic Fxs detection. If malignant bone neoplasms considered, CXR/CT, PET-CT to investigate metastatic spread and staging are important
Imaging Approach Bone Neoplasms
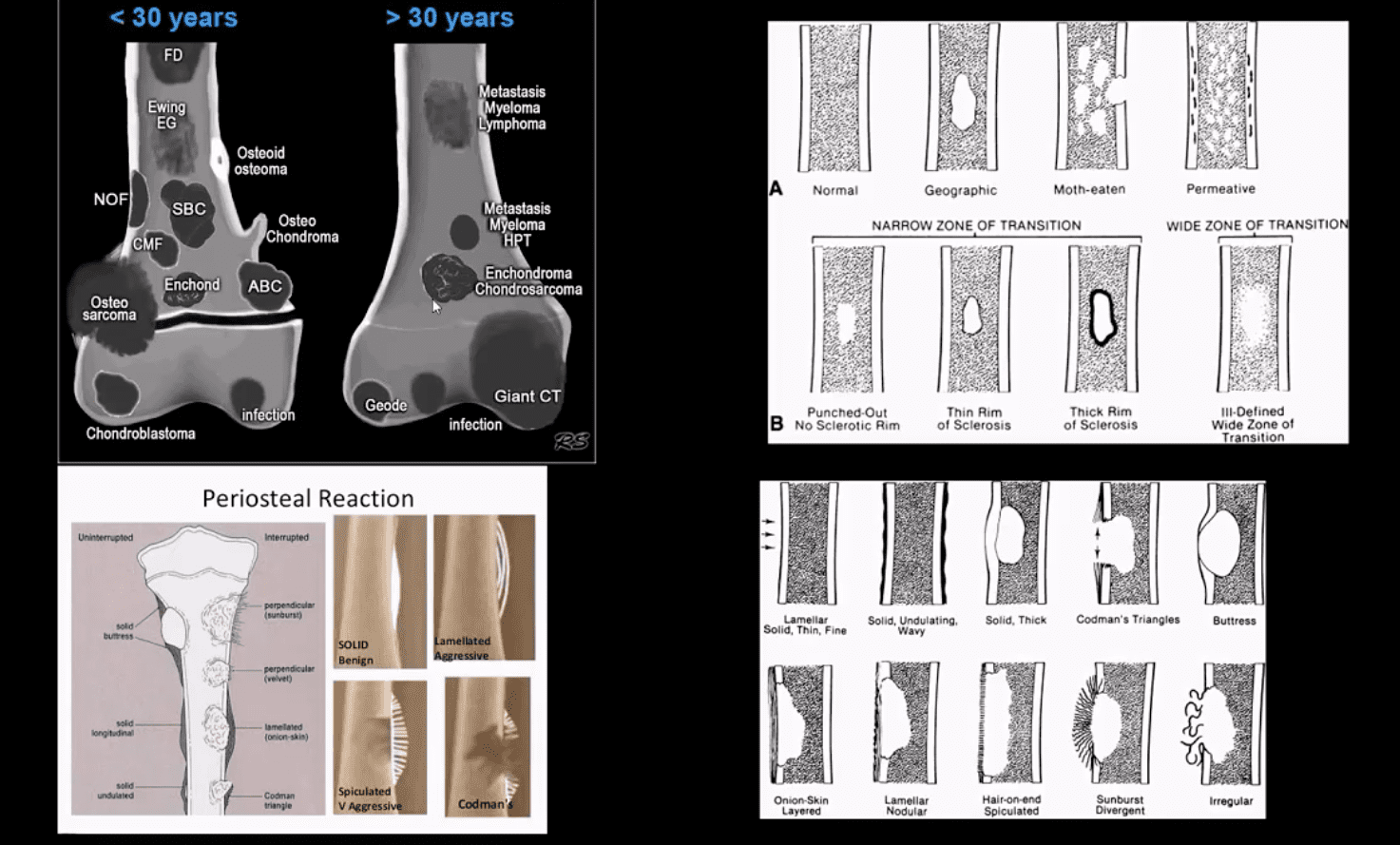
- Approach to imaging Dx of bone neoplasms includes age, bone location (epiphysis vs. metaphysis vs. diaphysis), a zone of transition surrounding the lesion, periosteal response, type of matrix, permeating or moth-eaten destruction vs. sclerotic, ground-glass, osteoid, cartilaginous matrix, soft tissue invasion, etc.
- Key x-radiography features to DDx benign vs. malignant bone neoplasm:
- Zone of transition: lesion is geographic with a narrow zone of transition vs. ill-defined wide zone of transition suggesting aggressive bone resorption
- What type of bone destruction occurred: soap-bubbly appearance vs. osteolytic vs. osteosclerotic changes
- Is there a round-glass matrix? Is there a well-defined rim of the sclerotic border with septations potentially suggesting slow growth and encapsulation like most benign processes.
- Periosteal proliferation: solid vs. aggressive spiculated/sunburst/hair-on-end with local soft tissue invasion and Codman triangle (study next slide)
FCD & NOF
- FCD & NOF or more appropriately Fibroxanthoma of the bone are benign bone processes that m/c seen in children. DDx based on the size with FCD presenting as <3-cm and NOF >3cm lesion composed of a fibrous heterogeneous matrix. FCD are asymptomatic and may regress in many cases. Some may progress to NOF. Location: identified in the knee region as an eccentric cortical based lesion.
- FCD must be DDx from an avulsive irregularity d/t repeated stress along Linea Aspera by extensors muscles
- Dx: radiography
- Management: leave-me-alone lesion. Occasionally NOF may progress and lead to pathologic fracture requiring an orthopedic consult
Osteochondroma
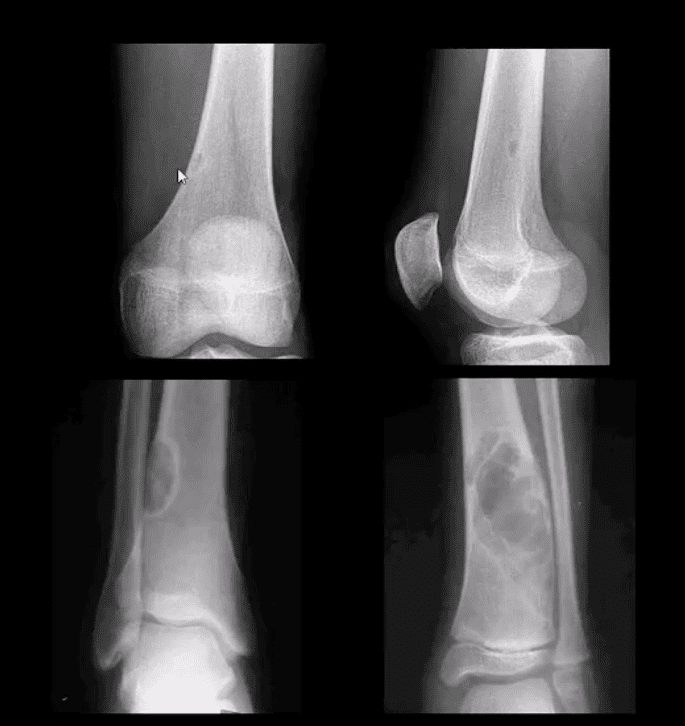
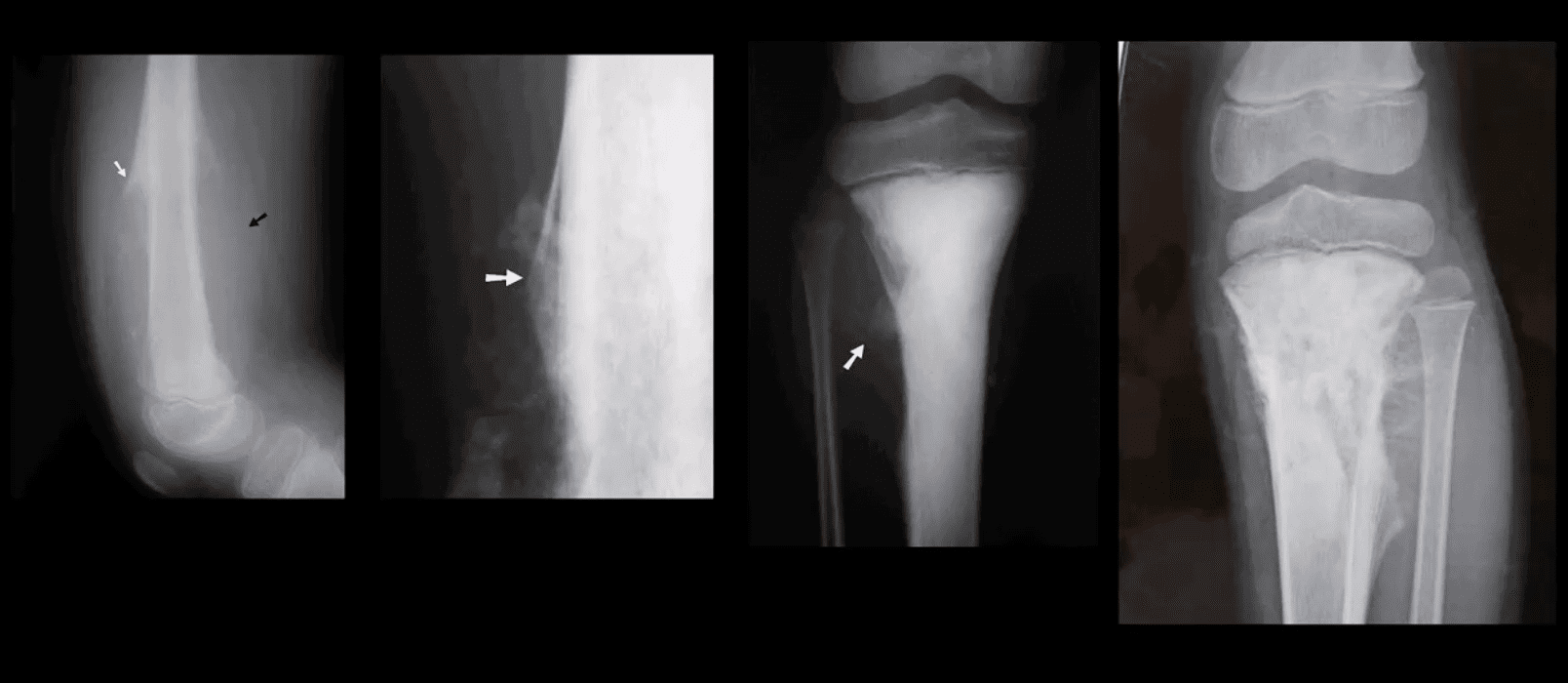
- Osteochondroma: m/c benign bone neoplasm. The knee is the m/c location. Contains all bone elements with a cartilaginous cap. Presented as pedunculated or sessile bone exostosis pointing away from the joint.
- 1% malignant degeneration to chondrosarcoma if solitary lesion and 10-15% in cases of HME
- Other complications: fracture (top left image) pseudoaneurysm of the Popliteal artery, adventitious bursa formation
- Hereditary Multiple Exostosis (HME)- autosomal dominant process. Presents with multiple osteochondromas (sessile-type dominates). May lead to limb deformities (Madelung deformity, coxa valga) reactive ST pressure, malignant degeneration
- Dx: radiography, MRI helps to Dx malignant degeneration to chondrosarcoma by changes in size and activity of cartilaginous cap (>2-cm in adults may manifest malignant degeneration). MRI will also help with Dx of regional complications
HME & Knee Pain
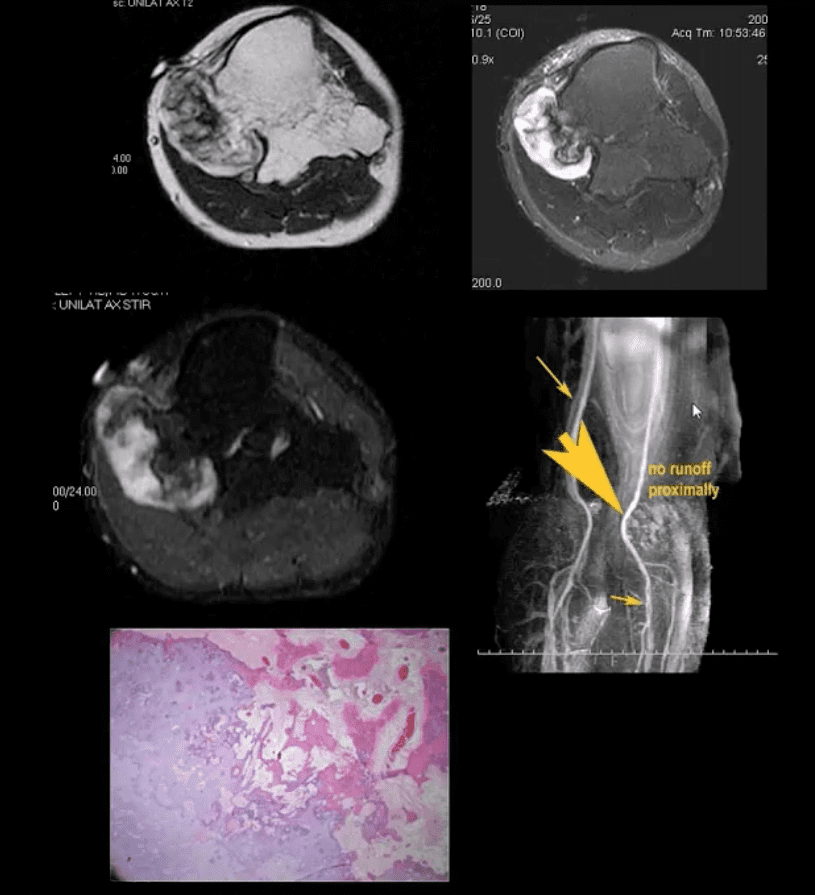
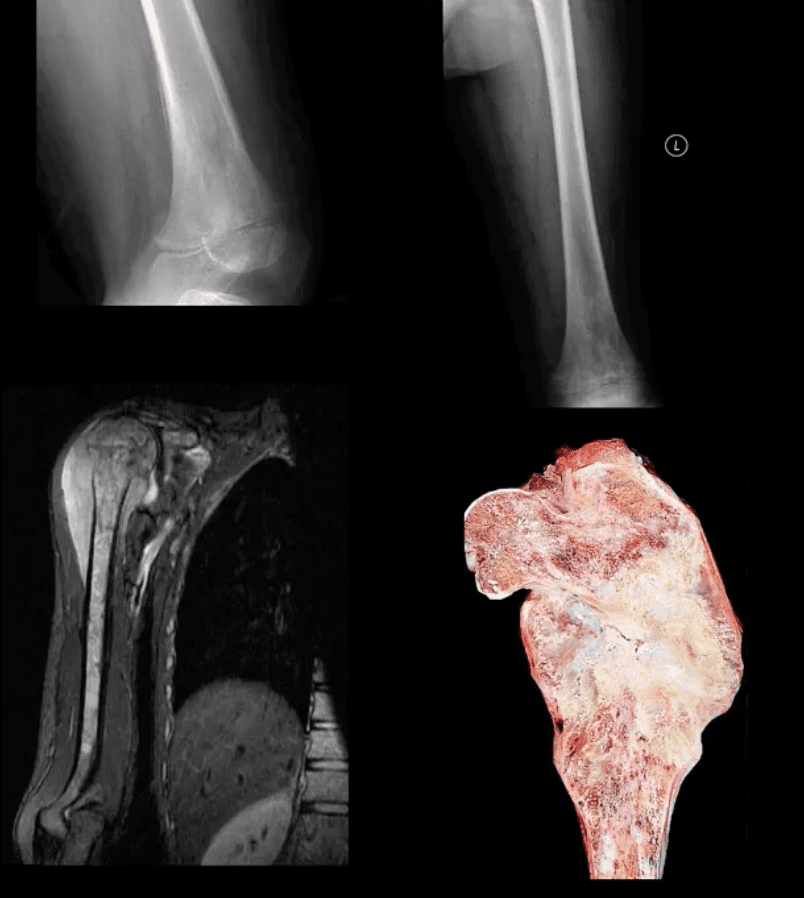
- 37-y.o male with HME and knee pain. Axial T1, T2 and STIR MRI slices at the popliteal region. Large cartilaginous cap and possible compression of the popliteal artery by osteochondroma. MRA was performed to evaluate popliteal A. pseudoaneurysm (large arrow). Pathology specimen obtained from the cartilaginous cap showed increased cellularity suggestive of malignant degeneration. Operative care was planned
Giant Cell Tumor (GCT) aka Osteoclastoma

- GCT- is a relatively common primary benign bone neoplasm. Age 25-40. M>F slightly.
- M/C location: Distal femur>proximal tibia>distal radius>sacrum
- GCT is the M/C benign sacral tumor. In 50% of cases, GCT occurs about the knee.
- GCT is histologically benign, but lung Mets may develop esp. if in distal radius and hands, often termed Malignant GCT
- <1% unresponsive/recurring GCTs may undergo malignant transformation to high-grade bone sarcoma
- Pathology: histologically composed of osteoclasts-multinucleated giant cells with stromal cells derived from precursors monocyte-macrophage type. Produces cytokines and osteolytic enzymes. GCT may contain blood and associated with secondary Aneurysmal Bone Cyst (ABC)
- Clinically: knee pain unresponsive to conservative care. Pathologic Fx may occur
- Imaging: always begins with radiography followed by MRI and surgical biopsy that are crucial to Dx.
- Rx: operative with curettage and cementing, a surgical appliance may be used if pathological fx present and cortical breach. In more severe cases other options available
Radiologic-Pathologic Dx
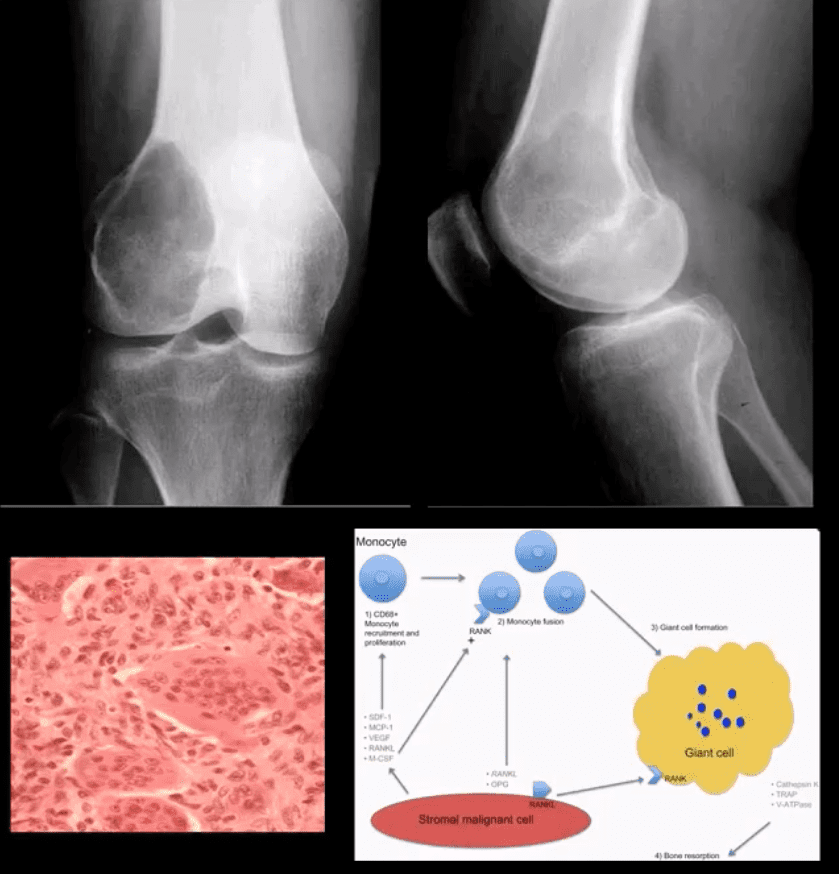
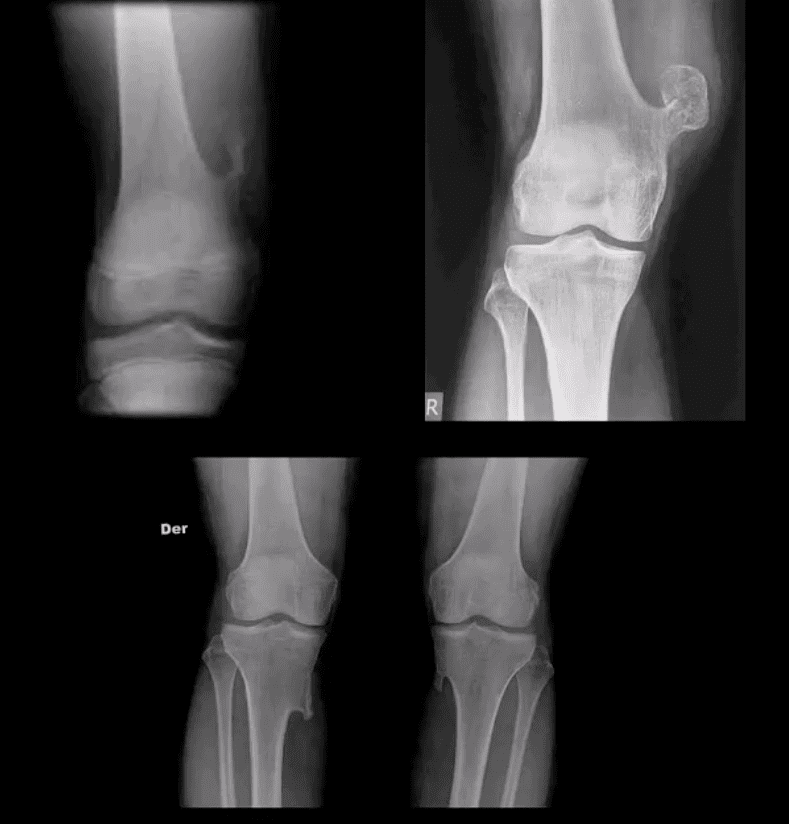
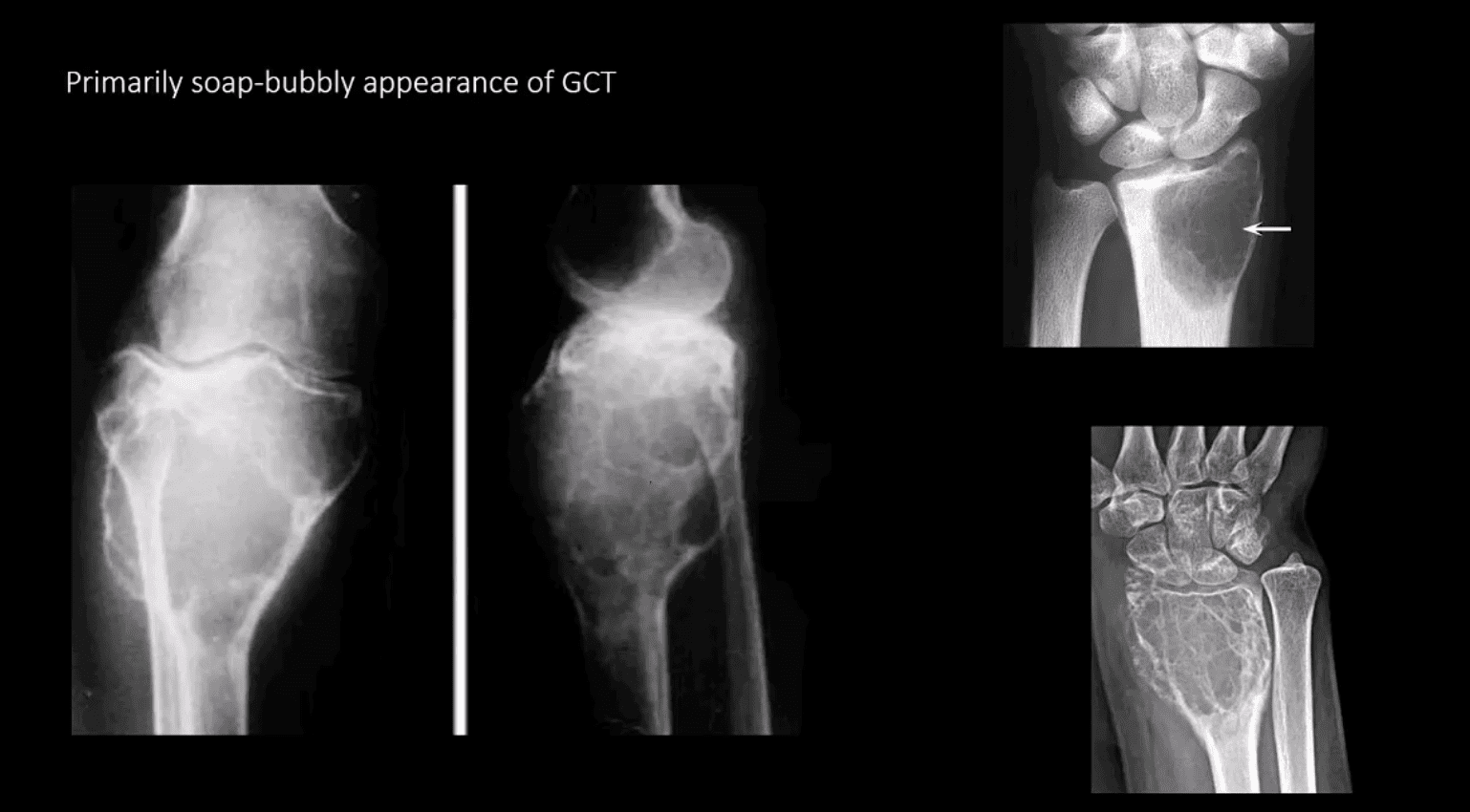
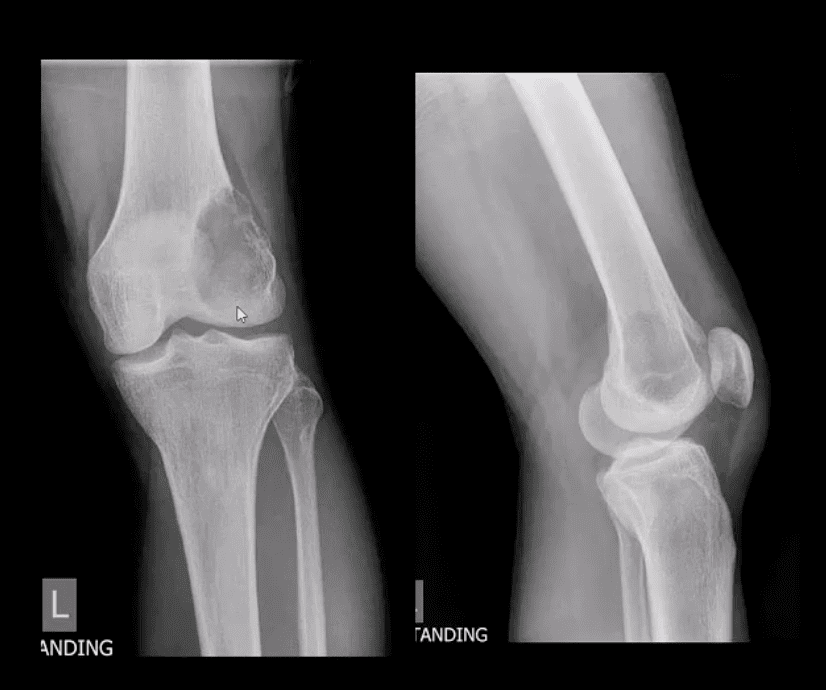
- Radiologic-pathologic Dx: osteolytic and/or soap-bubbly lesion typically involving metaphysis and into epiphysis (classic key feature) with subarticular extension. Zone of transition is generally narrow but occasionally in aggressive lesions wide zone of transition may be seen.
- MRI: low T1, highT2/STIR, characteristic fluid-fluid levels noted that are present in GCT and ABC. Histology is crucial to Dx.
- DDx: ABC, Brown cell tumor of HPT (osteoclastoma), Telangiectatic Osteosarcoma
- Radiological rule: if the physeal growth plate is present Dx of GCT is taken off the list in favor of chondroblastoma and vice versa.
Primarily Soap-Bubbly Appearance of GCT
Coronal, Fat-Sat Sagittal & Axial MRI Slices of GCT
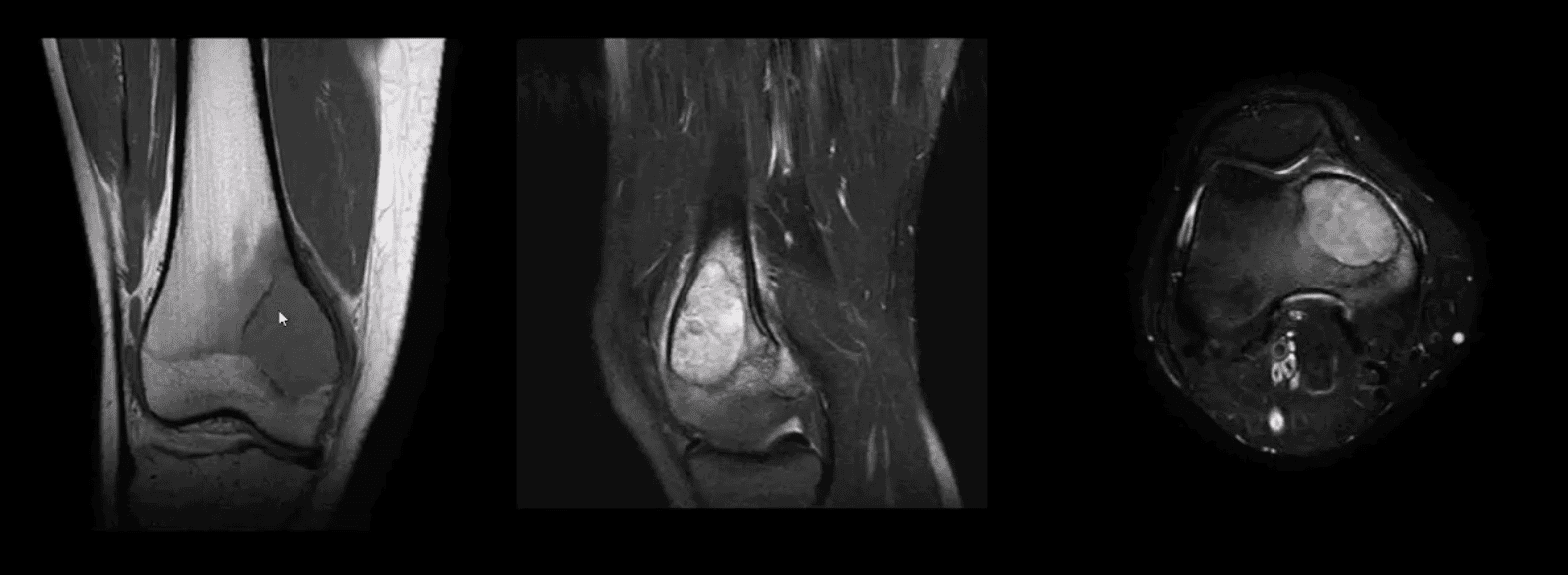
- T1 coronal, T2 fat-sat sagittal and T2 axial MRI slices of GCT. Typically: low T1, highT2/STIR and fluid-fluid levels
Characteristic MRI Appearance of GCT
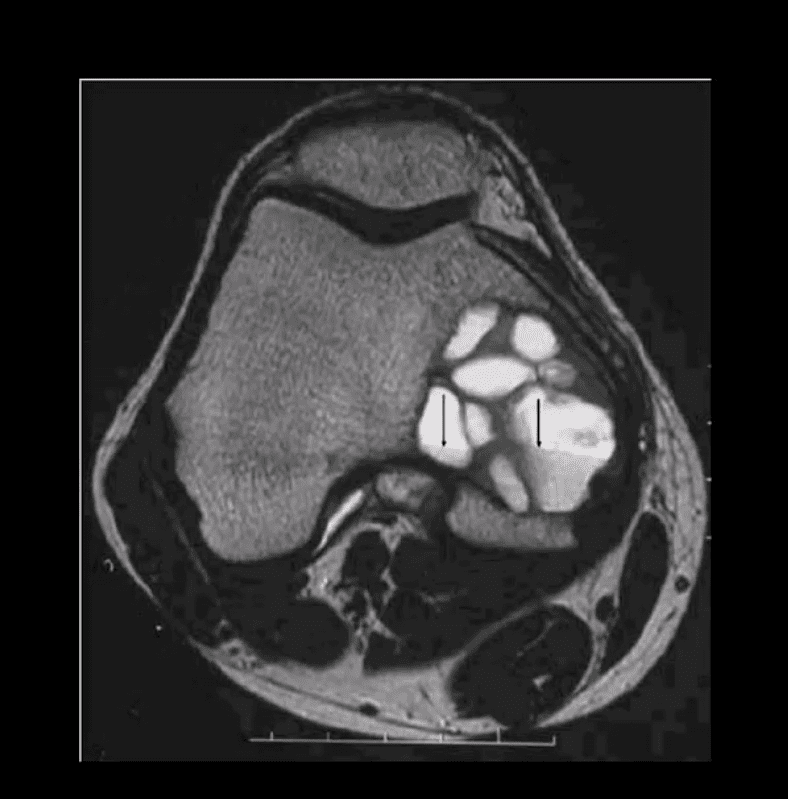
- Fluid-fluid levels d/t different composition of blood degradation products
- Important DDx: ABC
Malignant Neoplasms About the Knee
- In children and very young adults, the m/c primary malignant neoplasm is central aka intramedullary (osteogenic) osteosarcoma (OSA). Second peak of OS: >70 y.o d/t Paget’s (1%) and/or post radiation OSA.
- The knee is the m/c location of OSA (distal femur, prox. Tibia)
- The 2nd m/c malignant pediatric primary is Ewing sarcoma.
- In adults >40 y.o. the m/c primary is Multiple Myeloma (MM) or Solitary Plasmacytoma
- Overall m/c bone neoplasms in adults d/t bone Mets from lung, breast, prostate, renal cell, thyroid (discussed)
- Dx: clinical and radiological with surgical biopsy
- Imaging is crucial to Dx. 1st step x-radiography. MRI+ gad C is vital
- CT scanning occasionally helps to evaluate pathological fracture
Central (Intramedullary) Osteosarcoma (OSA)

- m/c age: 10-20. M/c location: knee, males>females. Increased risk in some
- congenital syndromes and mutation of the retinoblastoma gene: Rothmund-Thompson AR syndrome.
- Early Dx is important d/t 10-20% present with Lung Mets at Dx. Prognosis depends on stages. Early stages with local bone invasion and no
- mets 76% of survival.
- Rx: limb salvage procedures preferred with 8-12 weeks of chemo, amputation if encased neurovascular tissue, path Fx, etc.
- Imaging: radiography and MRI.
- Clinically: bone pain, Inc. Alkaline Phosphatase
- Chest CT if lung Mets considered
Classic Rad Features of OSA
- Osteoid forming a sclerotic mass with aggressive hair-on-end/speculated/sun-burst periosteal reaction, Codman's triangle and soft tissue invasion. Order MRI for staging and extent. Chest CT is crucial for Lung Mets dx.
MRI is Crucial for Dx/Staging
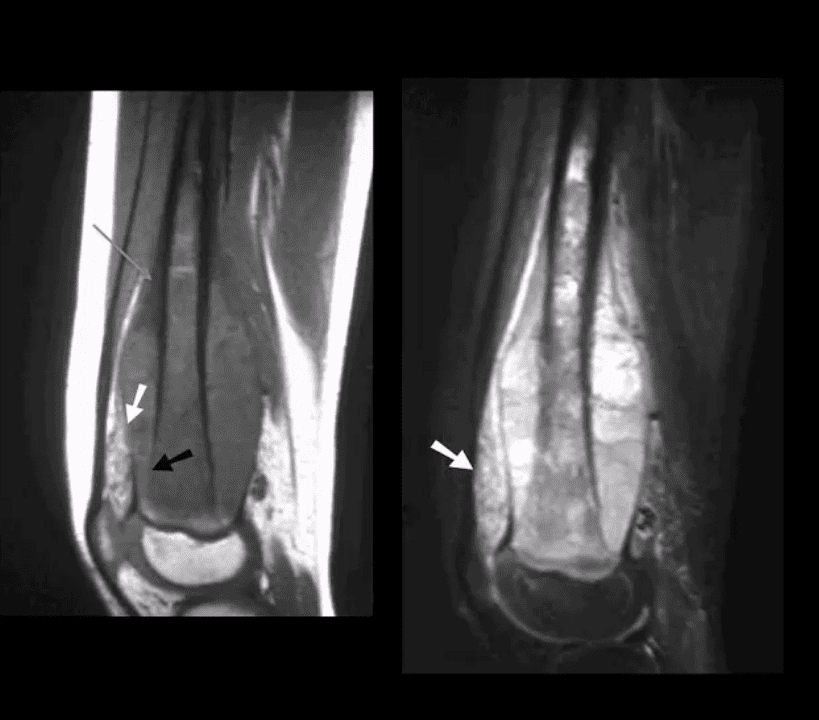
- Note sagittal T1 (left) and STIR (right) MR slices: large mass extending from distal femoral metaphysis to remaining shaft. A low signal on T1 and high on STIR d/t marrow invasion with edema, hemorrhaging and tumor invasion. Local ST invasion was seen (white arrows). Periosteal lifting and Codman’s triangle (green arrow) are additional signs of aggressive neoplasm.
- Note an interesting feature that the epiphysis is spared d/t physeal plate serving temporarily as an additional barrier to the tumor spread.
Ewing Sarcoma
- Ewing sarcoma: age: 2-20, uncommon in black patients. 2nd m/c highly malignant bone neoplasm in children that typically arises from the medullary cavity (Round cell tumors). Key symptom: bone pain that may mimic infection (ESR/CRP/WBC) Considered PNET
- Key Rad Dx: aggressive moth-eaten/permeative lucent lesions in the shaft of long bones with large soft tissue invasion/typical onion skin periostitis. May produce saucerisation
- May affect flat bones. May appear as sclerotic in 33%. Early lung Mets (25-30%) bone-to-bone Mets
- Poor prognosis if delayed Dx. Imaging steps: 1st step x-rad, MRI is v. important followed by a biopsy. CXR/CT PET-CT
- Rx: combined rad-chemo, operative.
M/C Malignant Knee Neoplasms in Adults
- 66-y.o. male with knee pain
- Note aggressive expansile osteolytic lesion in the distal femur metaphysis into epiphysis. No periosteal reaction present. Following further work up with abdominal and chest CT scanning, Dx of Renal cell carcinoma was established
- Distal Mets into lower extremity are more common with lung, renal cell, thyroid and breast CA.
- Renal cell and Thyroid will typically present with aggressive osteolytic expansile mass aka “blowout Mets.”
- In general, imaging approach should consist of Radiographic knee series, followed by MRI if x-rays are unrewarding
- Tc99 Bone scintigraphy is the modality of choice to evaluate metastatic bone disease
Soft Tissue Neoplasms About the Knee
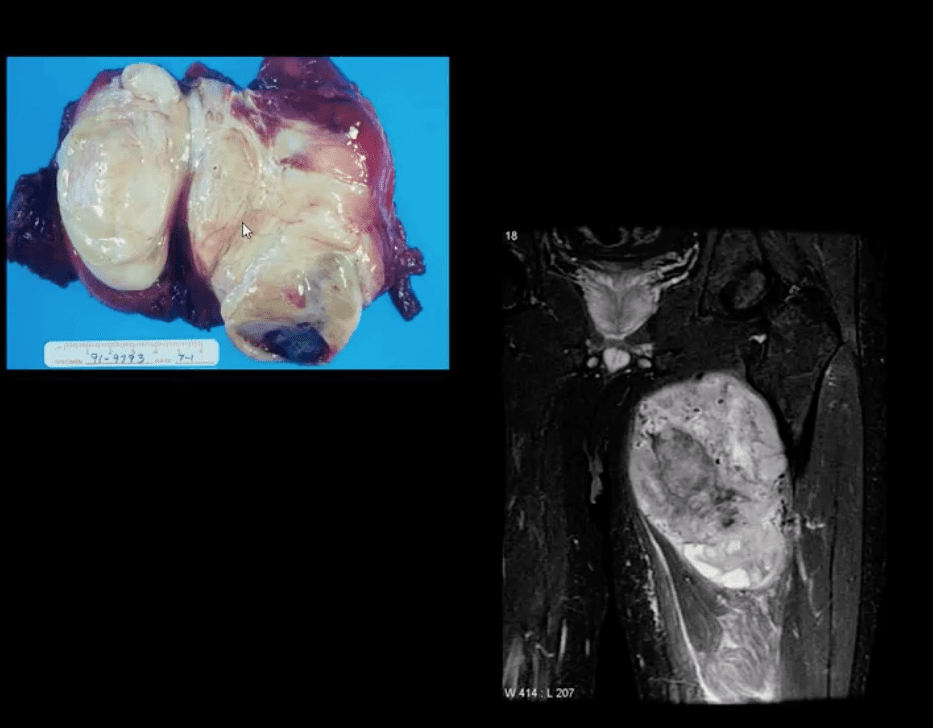
- Malignant fibrous histiocytoma (MFH) reclassified as Pleomorphic Undifferentiated Sarcoma (PUS) is the m/c S.T. sarcoma. MFH is aggressive biologically with poor prognosis
- M>F (1.2:1) 30-80 with a peak in a 6th decade. 25-40% of all adults sarcomas m/c extremities. Retroperitoneum next (worst prognosis d/t late Dx and large growth w/o symptoms)
- Clinically: painful, hard mass typically about the knee or thigh. Histology: poorly differentiated/undifferentiated malignant fibroblasts, myofibroblasts and other mesenchymal cells
- Imaging: MRI is the modality of choice with T1, T2, T1+C. Typically appears as an aggressive heterogeneous mass intermediate to low signal on T1 and high signal on T2 with areas of necrosis and enhancement on T1+C. May appear misleadingly encapsulated w/o true capsule
- Management: operative with radiation and chemotherapy. Tumour depth is crucial for prognosis. 80% 5-year survival if <5cm deep in ST and 50% if >5-cm deep in ST.
Synovial Sarcoma

- Synovial sarcoma: common malignant ST neoplasm esp. in younger patients or older children/adolescents. M/C found in the knee area
- Clinically: can present slowly as a palpable mass in the extremity often ignored the d/t slow growth
- Imaging is the key: radiography may reveal ST. density/mass. Some synovial sarcomas may show calcification and mistaken for Myositis Ossificanse or heterotopic bone formation
- MRI with T1, T2, and T1+C are Dx modality of choice. Other modalities: US, CT are non-specific
- DDx: MFH
- Management: operative, chemo-radiation
- Prognosis: variable depending on size, invasion, metastasis
For Complete List Of Bone & Soft Tissue Neoplasms
- http://bonetumor.org
- Further reading:
- https://emedicine.medscape.com/article/988516-differential
- https://www.ajronline.org/doi/10.2214/AJR.16.17434
- For further review of common childhood malignancies refer to:
- https://www.aafp.org/afp/2000/0401/p2144.html
