




Hyperextension Injury
- Hangman's Fx aka traumatic spondylolisthesis of C2 with a fracture of pars interarticularis or pedicles (unstable)
- MVA is the most common cause
- Mechanism: acute hyperextension of upper C/S similar to judicial hanging (never actually seen and most deaths are due to asphyxiation)
- Secondary flexion may tear PLL and disc
- Associated injuries: 30% have other c-spine fx especially Extension teardrop at C2 or C3 due to avulsion by ALL
- Cord paralysis may only present in 25% due to bony fragments dissociation and canal widening
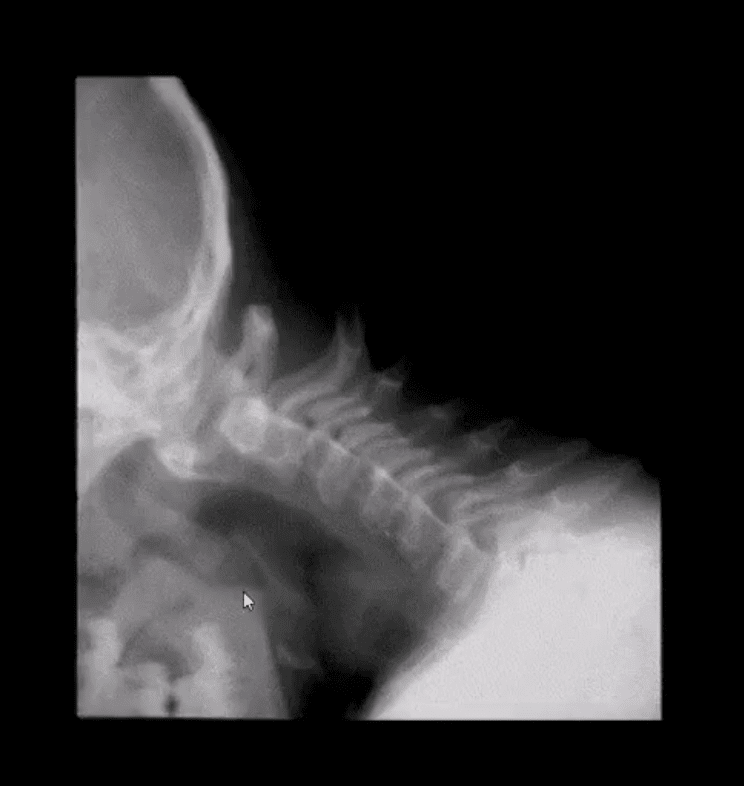
- Hangman fx and extension teardrop
- Cervical degeneration and previous fusion is a key predisposing factor due to the lack of mobility and suppleness, rendering C/S easy to fracture
- Imaging: initial x-radiography then CT that helps to delineate another injury such as facet/pedicle Fx further. MRI may help if complicated by Vertebral A. damage
- Management: if type 1 injury then closed reduction and rigid collar for 4-6 weeks, halo bracing if type 2 (>3-5mm displacement) Fx/instability, anterior or posterior spinal fusion at C2-3 if type 3 Fx (>5-mm displacement)
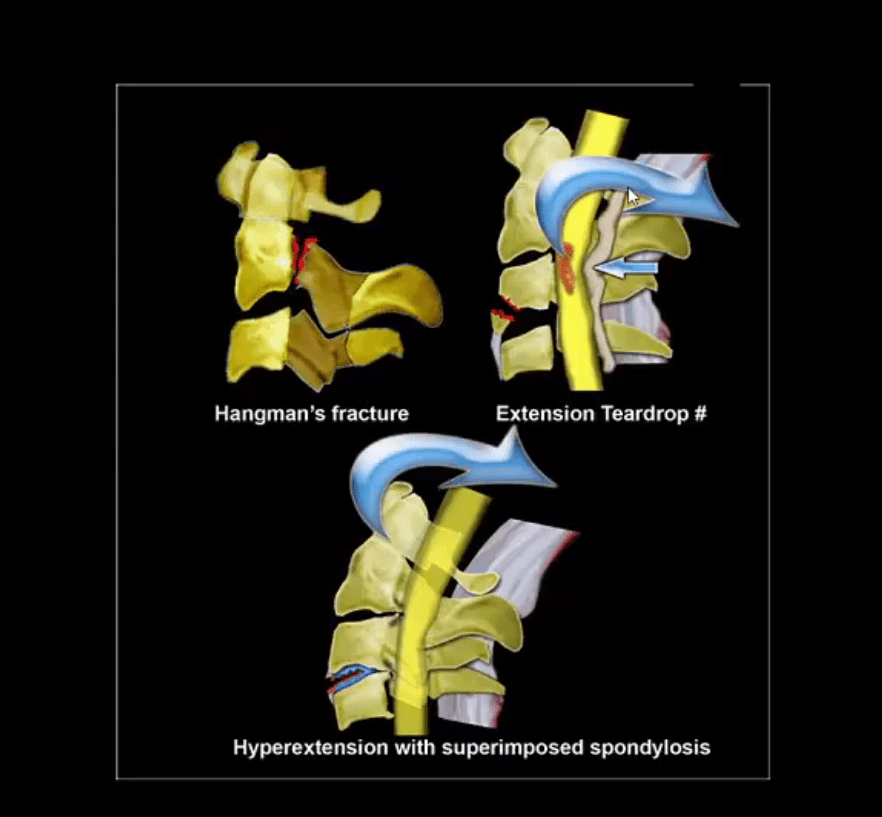
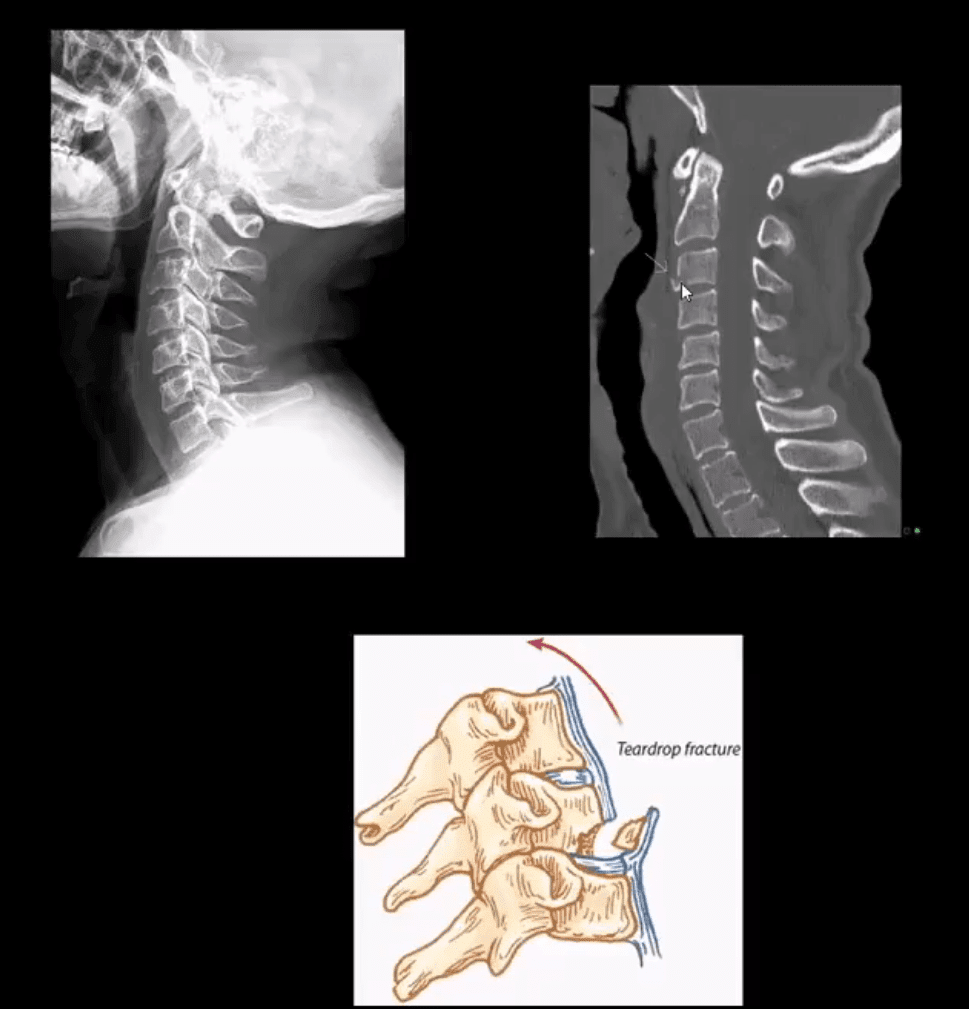
- Extension teardrop Fx (stable) potentially unstable if put in extension
- Avulsion of an inferior anterior body by ALL. More seen in elderly with superimposed C/S spondylosis
- Key radiography: a smaller anterior-inferior body corner, no disruption of ligamentous alignment. Typically at C2 or C3 due to sudden hyperextension and ALL avulsion
- Complication: central cord syndrome (m/c incomplete cord injury) esp. in superimposed spondylosis and canal stenosis by the laxity of ligamentum flavum and osteophytes
- Management: hard collar isolation
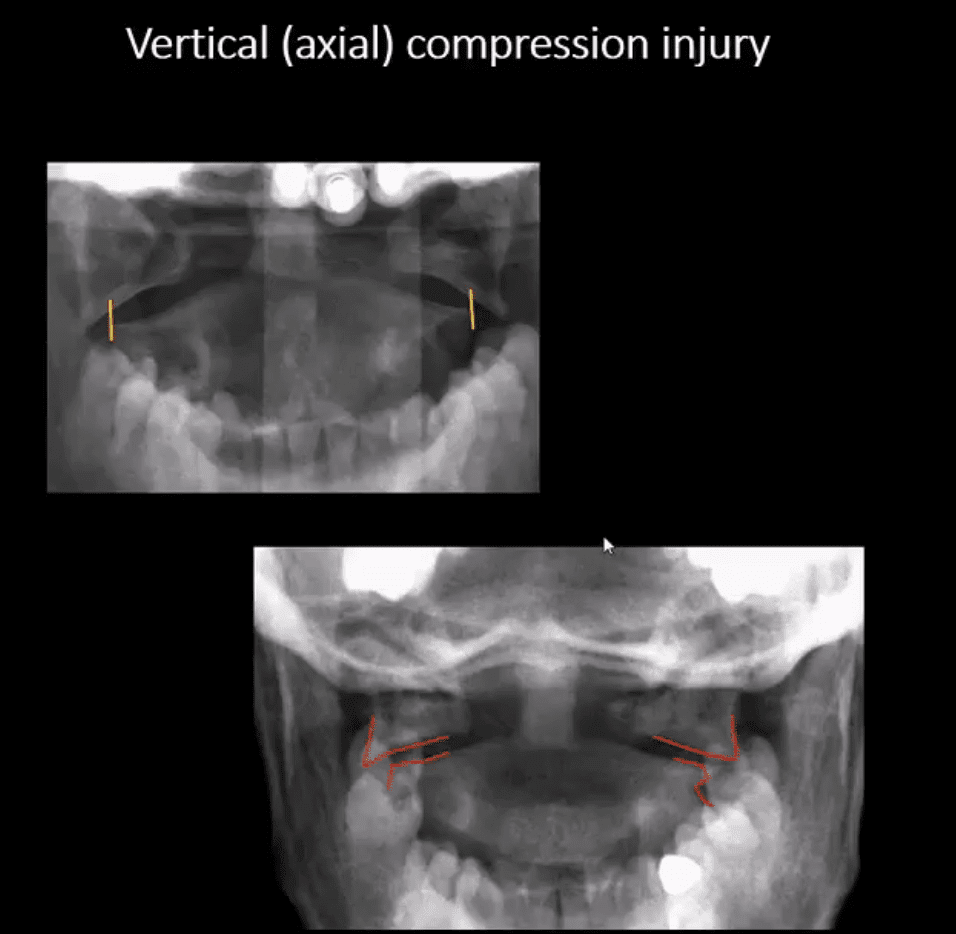
Vertical (axial) Compression Injury
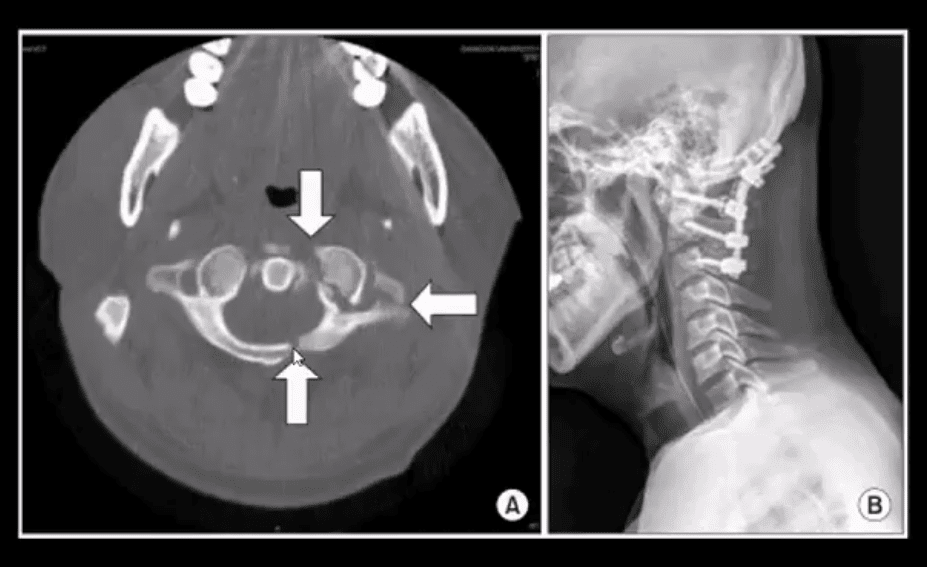
- Jefferson Fx (named after British neurosurgeon who defined it) (unstable but neurologically intact Fx) 7% of all C/S injuries. Stability is dependent if the transverse ligament is intact or torn, which can be noted by overhanging of C1 lateral masses over C2 >5-mm combined (left image)
- Mechanism: C1 compression (e.g., diving into shallow waters) causing burst Fx-classically 4-parts of the anterior and posterior arch of C1. Variations exist.
- Complications: 50% show other C/S Fx, 40% show Odontoid C2 Fx esp. if extension and axial loading occur
- Imaging: x-radiography followed by CT scanning to evaluate subaxial injury and complexity of C1 injury. Note Jefferson Fx with pillar and transverse foramina fx requiring posterior occipital-cervical fusion (below right image).
- Management: rigid collar immobilization if the transverse ligament is intact. Halo brace or fusion if the transverse ligament is ruptured
Cervical Injuries With Variable Mechanisms of Trauma
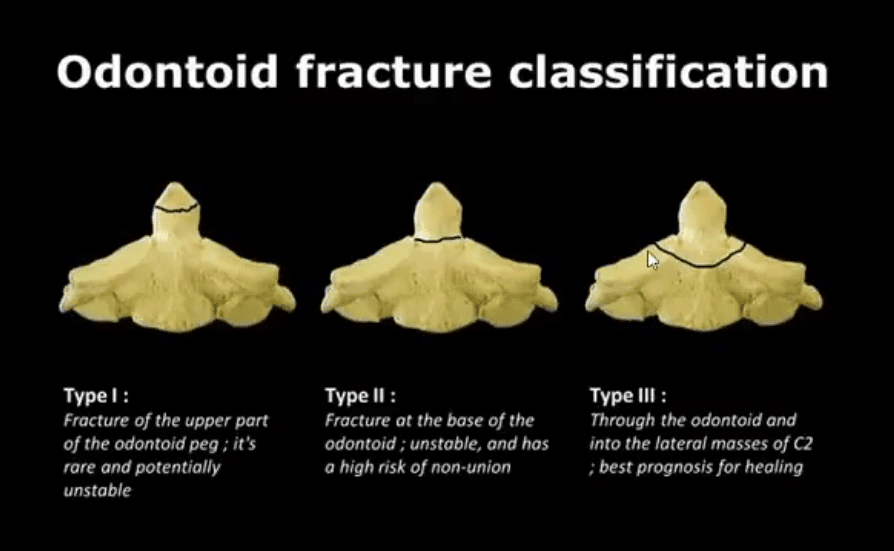
- Odontoid process fractures:
- These occur with a variety of mechanisms, flexion, extension, lateral flexion. Elderly with superimposed spondylosis are at higher risk.
- Anderson & D'Alonzo classification (below). Type 2 is the most common and most unstable. Type 3 has the best chance of healing d/t more massive bleed into C2 body and better healing potential.
- Imaging: x-radiography can miss some Fx. CT scanning is essential.
- On x-radiography note tilting of the Dens on lateral and APOM views. CT will reveal the injury and classify it.
- Complications: cord injury, non-union
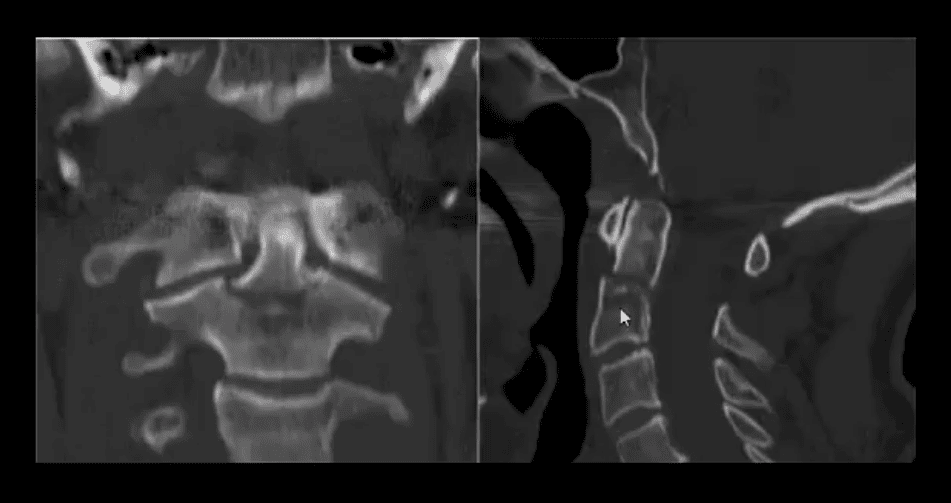
- CT scanning: type 2 odontoid fracture (unstable)
- Management: type 1 (alar ligament avulsion) most stable observed and treated with rigid collar.
- In young patients, Halo brace is used to treat type 2
- Older patients do not tolerate Halo
- Operative C1-2 fusion if unstable is Dx and cord signs or other complicating factors are present
Normal Radiographic Variants & Anomalies Simulating Pathology
- Pediatric spine appears different especially in children younger than 10-years old.
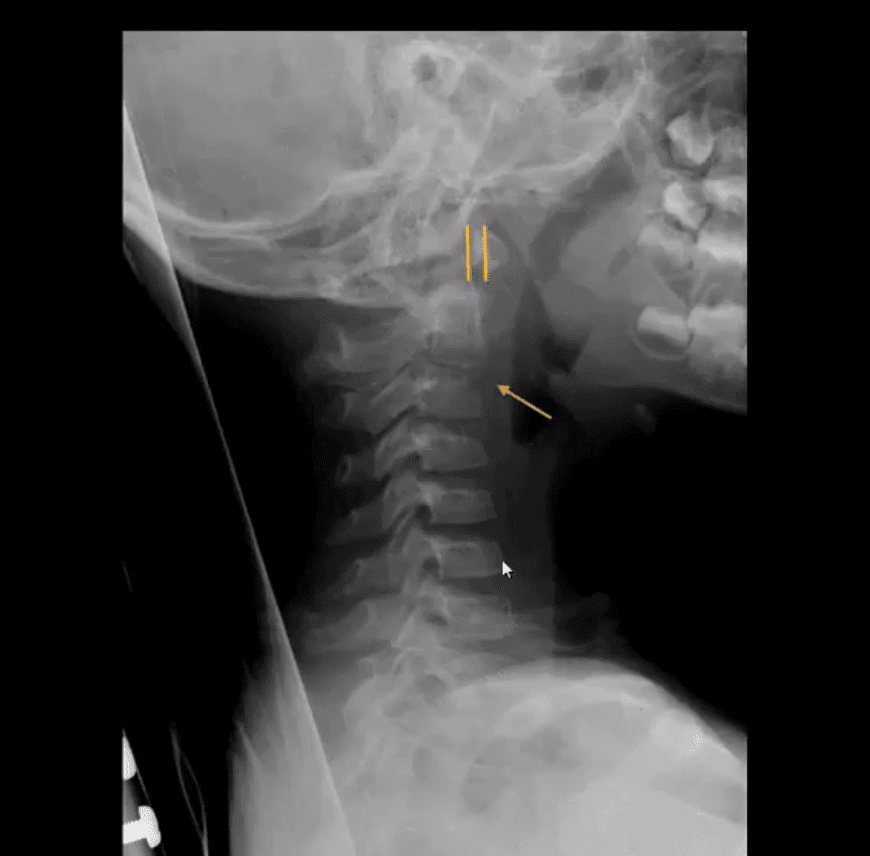
- Normal variations; ADI 5-mm and may increase or decrease on flexed/extended views by 1-2-mm
- C2-3 may appear as pseudo-subluxation due to normal ligamentous laxity in children (below arrow)
- Pediatric vertebral bodies usually are narrower and anteriorly wedged due to the presence of cartilaginous tissue
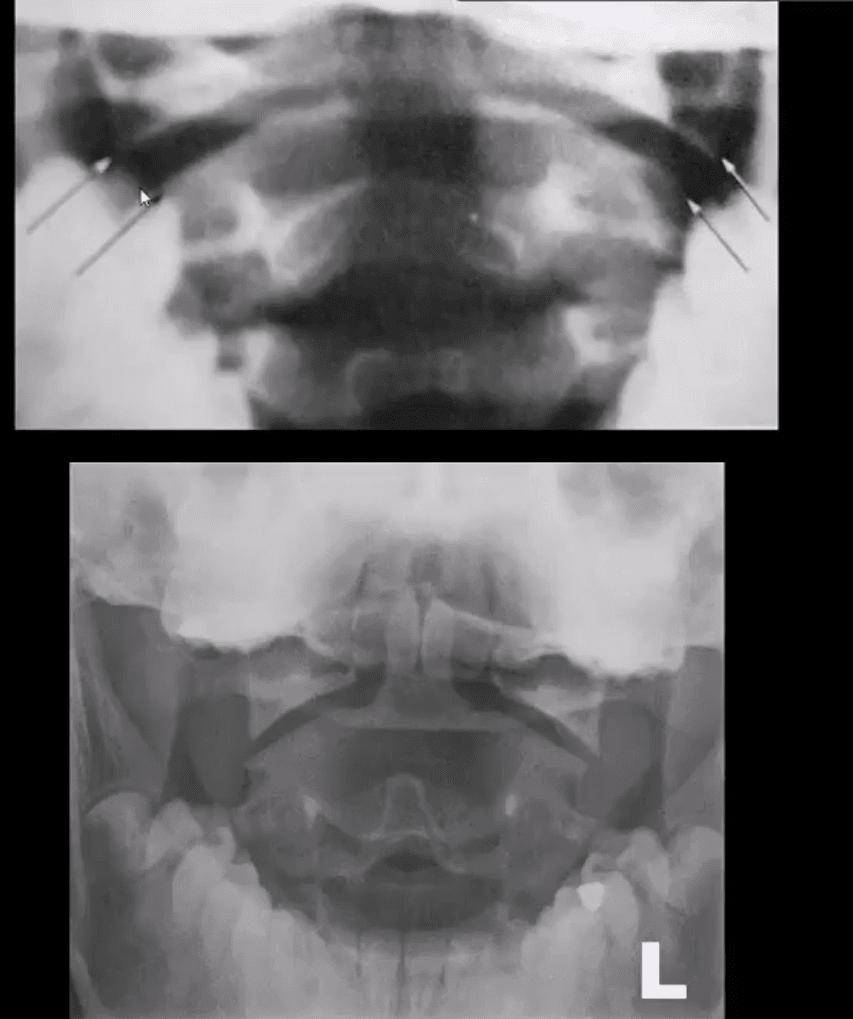
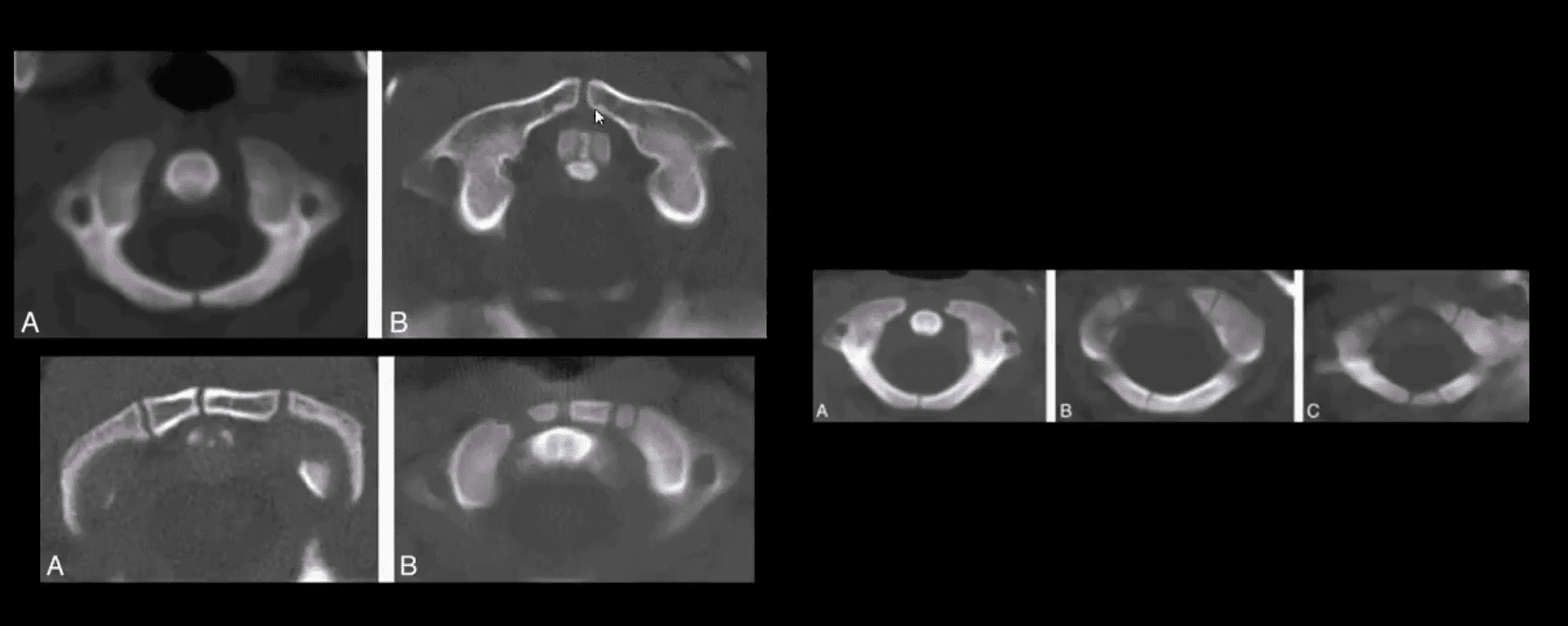
- APOM view appears different in children, and some asymmetry of C1 articular masses is normal (below top image) and should not be confused with Jefferson Fx
- In adults, any asymmetry or "overhanging" of C1 articular masses is pathological and may indicate Jefferson fx
- Standard ossification centers of the Atlas synchondrosis in children should not be mistaken for fractures
- Persistent ossiculum terminal of Bergman is a typical variant/anomaly of tenacious un-united ossification center and should not be confused with type odontoid fx
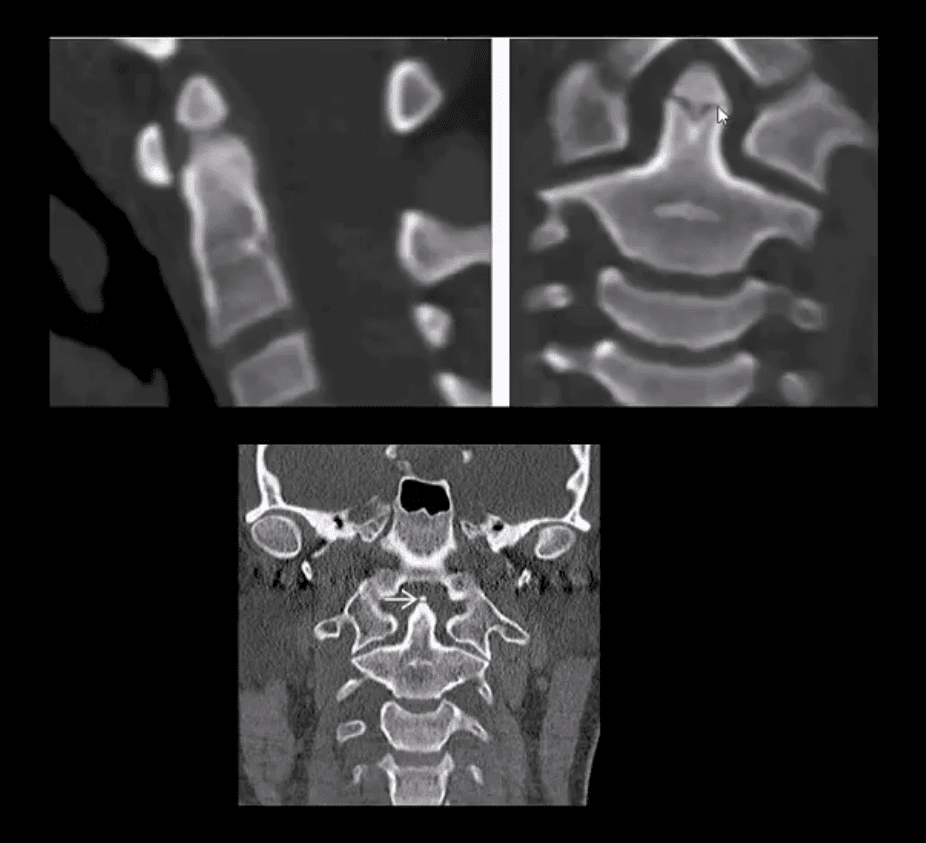
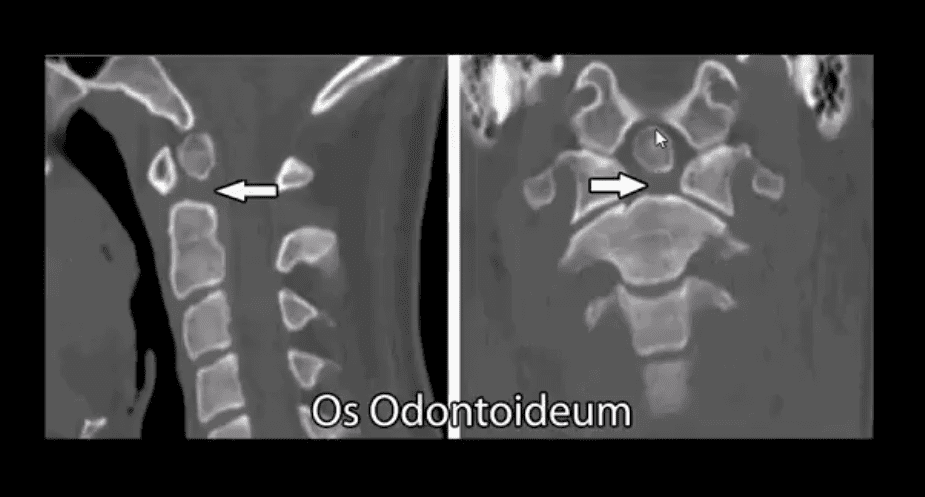
- Os odontoideum
- Un-united growth center that currently considered as an un-noticed injury that disturbed normal growth in a child younger than 5-years-old
- It may be a cause of C1-2 instability and should be evaluated with flexed and extended cervical views
- Should not be confused with type 2 Dens fracture because it typically more demonstrates greater mineralization of bone
- Incomplete bilateral agenesis of the C1 posterior arch
- Anomalous closure of C1 posterior arch
- Should not be confused with a fracture
- However, local or cord symptoms may develop after trauma in some cases
- Relatively rare anomaly developing due to failed chondrogenesis and ossification of posterior ossification centers of the Atlas
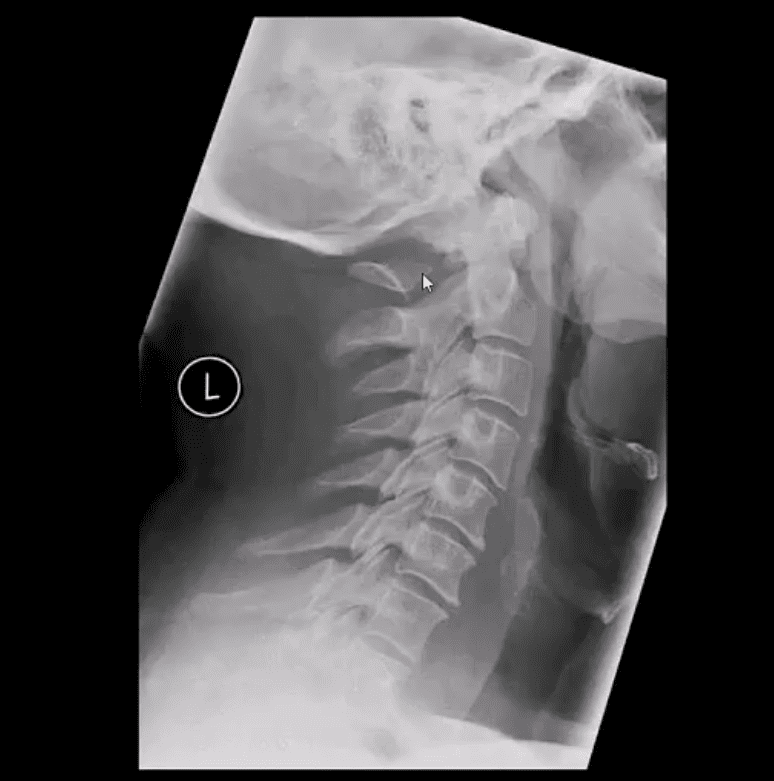
- Patients with Down syndrome may suffer from increased ligamentous laxity and other abnormalities
- Increased risk of subluxation at C1-2
- Burst Fx (unstable) 2-columns are damaged
- Mechanism: axial loading with frequent flexion after falls and MVAs
- The thoracolumbar region is the most vulnerable due to the increased fulcrum of motion
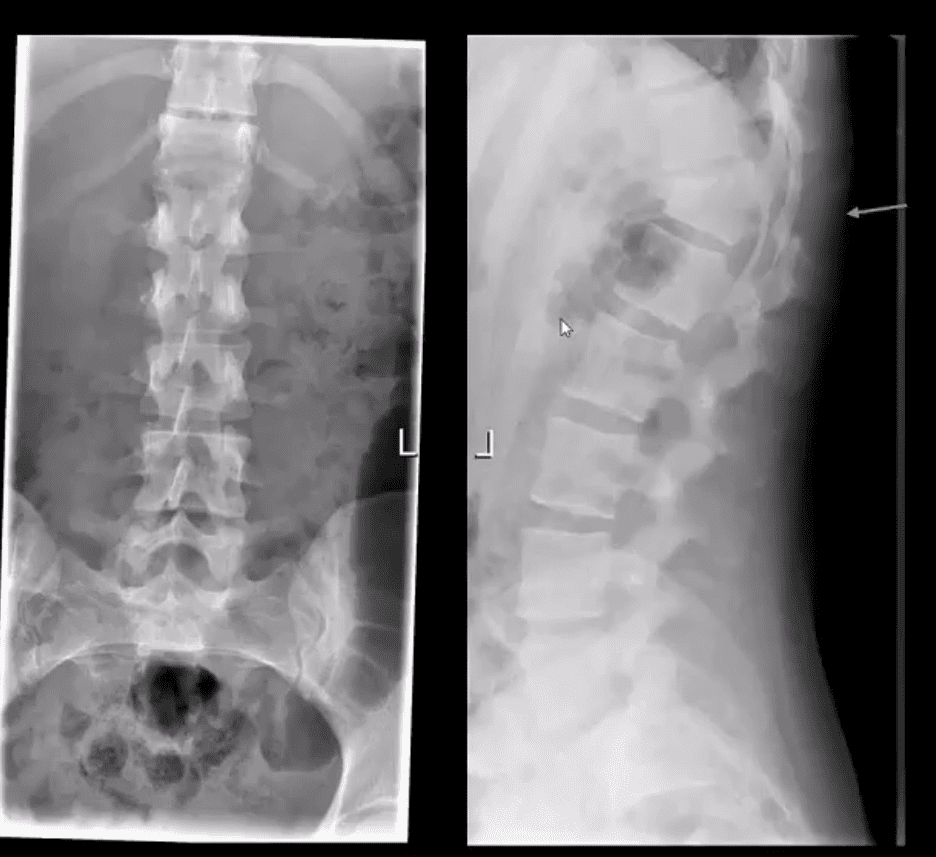
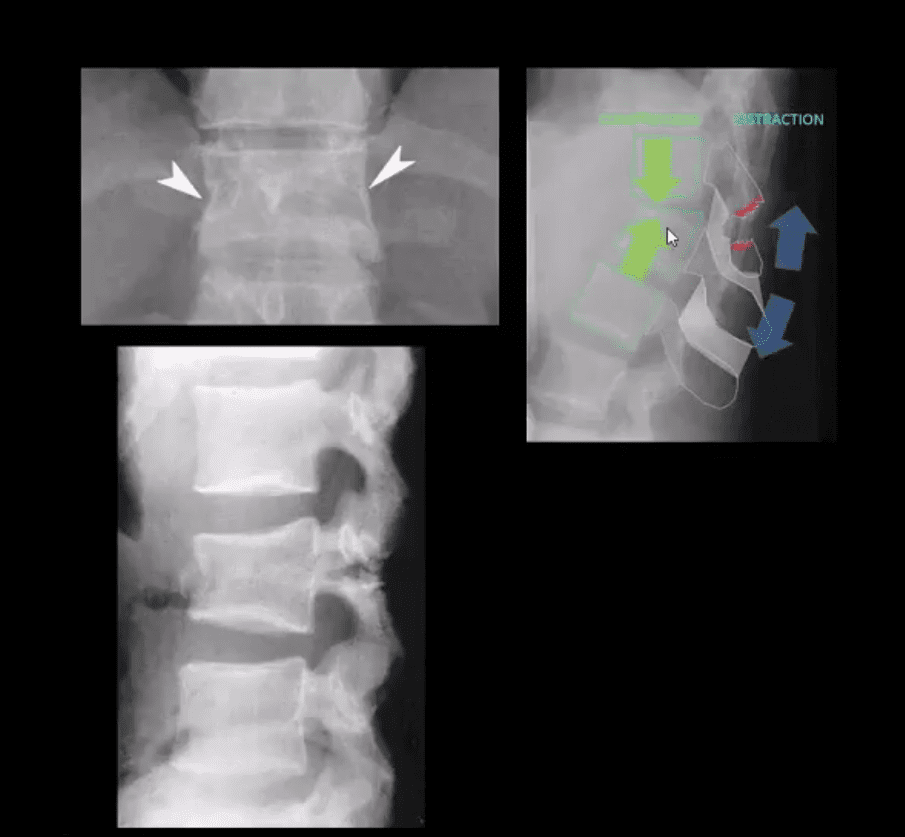
- Key radiography: acute compression fracture and collapse of body height, retropulsion of posterior body and acute kyphotic deformity on the lateral view
- On the frontal view: interpedicular widening (below yellow arrow), regional soft tissue swelling (below green arrow)
- Imaging: x-radiography should be followed by CT scanning w/o contrast
- MRI if neurologically unstable due to cord or conus injury
- Complications: cord damage by acutely retropulsed bone fragments
- Management: non-operative if neurologically intact and <50% body retropulsed with minimal kyphosis
- Operative (fusion) if 50% or more body retropulsed, laminar/pedicle Fx, neuro compromised
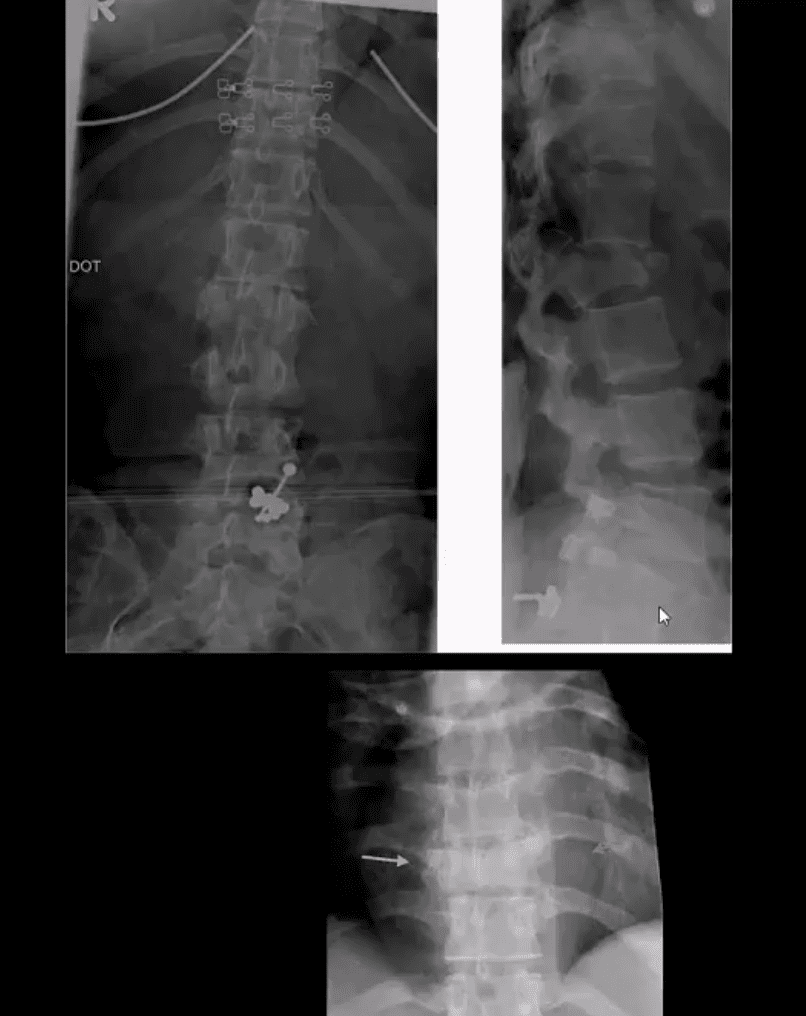
18-Year Old Female Following Trampoline Accident
- AP & lateral L/S views
- Note acute compression fracture, a vertebral body extending to posterior elements
- Widening of the inter-spinous distance between T11-T12 (below arrow)
- Radiolucent fracture line is seen through the T12 body on the AP projection
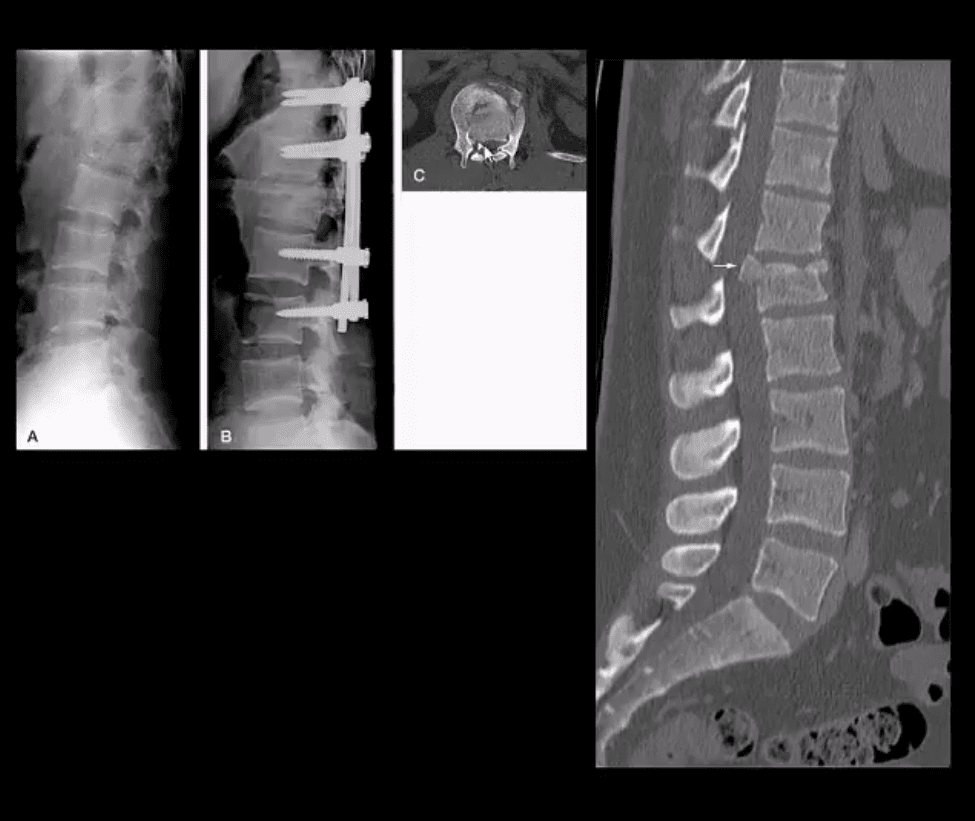
- CT scanning was performed
- Sagittal reconstructed Thoracic and Lumbar CT slices in bone window
- Note acute compression fracture, the T12 body extending into pedicle and lamin
- Dx: Chance fracture of T12
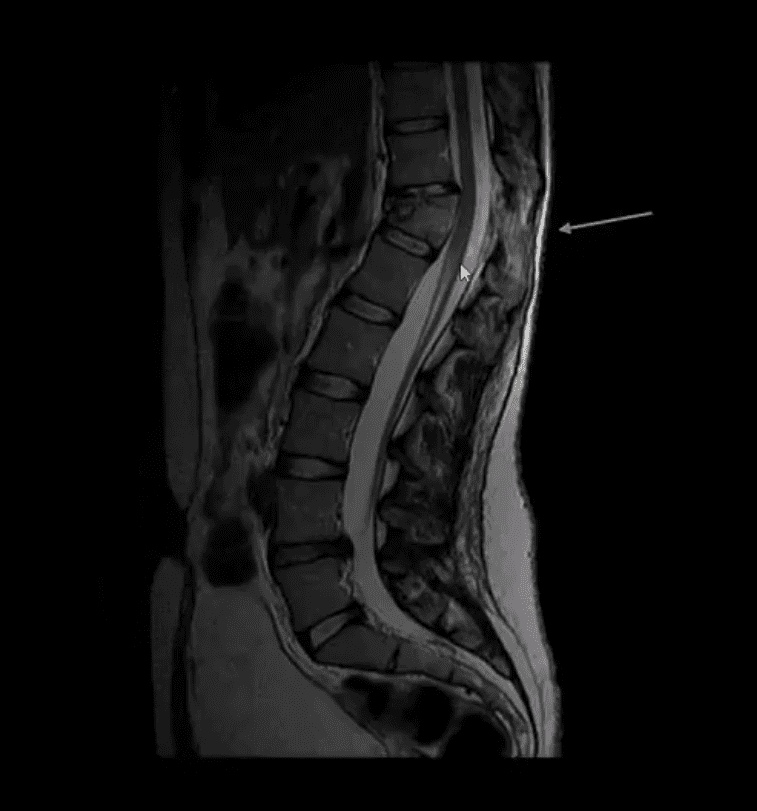
- MR imaging was performed

- T2 Wl sagittal MRI
- Findings: acute compression fracture T12 body extending to posterior elements causing rapture of interspinous and flavum ligaments
- Mild compression of the distal cord above the conus is noted with a minimal signal abnormality
- Dx: Chance fracture
- Chance Fx aka (Seatbelt Fx) - is a flexion-distraction injury (unstable)
- M/C in lower thoracic-upper lumbar
- All 3-columns fail: column 3 torn by distraction, columns 1 and 2 fail on compression (Denis classification)
- Causes: MVA, falls
- Imaging: initial x-radiography should be followed by CT scanning w/o contrast to assess bone fragments retropulsion/canal compression. MRI may help to evaluate potential cord damage and ligaments tearing
- Management: non-operative immobilization if neuro intact
- Operative decompression and fusion
Spinal Trauma Imaging Approach
Resources:
- https://emedicine.medscape.com/article/824380-overview
- https://emedicine.medscape.com/article/248236-overview#a9
- https://emedicine.medscape.com/article/397896-overview#a3
- https://www.aafp.org/afp/1999/p331.html
