




Imaging diagnostics are an essential element in the evaluation of spine trauma. Over the last few decades, the rapid evolution of imaging technology has tremendously changed the assessment and treatment of spinal injuries. Imaging diagnostics utilizing CT and MRI, among others, are helpful in the acute and the chronic settings. Spinal cord and soft-tissue injuries are best evaluated by magnetic resonance imaging, or MRI, whereas computed tomography scanning, or CT scans, best evaluate spinal trauma or spine fracture. The purpose of the article below is to demonstrate the significance of imaging diagnostics in spine trauma.
Cervical Spine Fracture Evaluation
Practice Essentials
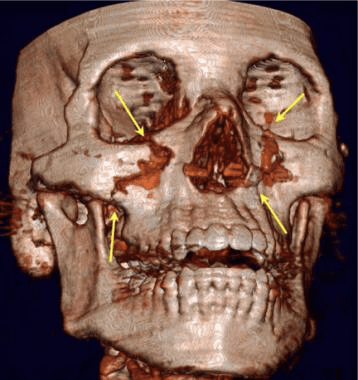
Approximately 5-10% of unconscious patients who present to the ED as the result of a motor vehicle accident or fall have a major injury to the cervical spine. Most cervical spine fractures occur predominantly at two levels: one-third of injuries occur at the level of C2, and one-half of injuries occur at the level of C6 or C7. Most fatal cervical spine injuries occur in upper cervical levels, either at craniocervical junction C1 or C2. [1, 2, 3, 4, 5, 6, 7, 8]
Anatomy
The normal anatomy of the cervical spine consists of 7 cervical vertebrae separated by intervertebral disks and joined by a complex network of ligaments. These ligaments keep individual bony elements behaving as a single unit. [7]
View the cervical spine as three distinct columns: anterior, middle, and posterior. The anterior column is composed of the anterior longitudinal ligament and the anterior two-thirds of the vertebral bodies, the annulus fibrosus and the intervertebral disks. The middle column is composed of the posterior longitudinal ligament and the posterior one-third of the vertebral bodies, the annulus, and intervertebral discs. The posterior column contains all of the bony elements formed by the pedicles, transverse processes, articulating facets, laminae, and spinous processes.
The anterior and posterior longitudinal ligaments maintain the structural integrity of the anterior and middle columns. The posterior column is held in alignment by a complex ligamentous system, including the nuchal ligament complex, capsular ligaments, and the ligamenta flava.
If one column is disrupted, other columns may provide sufficient stability to prevent spinal cord injury. If two columns are disrupted, the spine may move as two separate units, increasing the likelihood of spinal cord injury.
The atlas (C1) and the axis (C2) differ markedly from other cervical vertebrae. The atlas has no vertebral body; however, it is composed of a thick anterior arch with two prominent lateral masses and a thin posterior arch. The axis contains the odontoid process that represents fused remnants of the atlas body. The odontoid process is held in tight approximation to the posterior aspect of the anterior arch of C1 by the transverse ligament, which stabilizes the atlantoaxial joint. [9, 7]
Apical, alar and transverse ligaments provide further stabilization by allowing spinal column rotation; this prevents posterior displacement of the dens in relation to the atlas.
In pediatric patients, the spine is more flexible, and therefore, neural damage occurs much earlier than musculoskeletal injury in young patients. Because of this high flexibility, fatal consequences can occur with sometimes even minimal structural damage. Compared to adults, children have a different fulcrum because of a relatively large head, the vertebrae are not completely ossified, and the ligaments are firmly attached to articular bone surfaces that are more horizontal, making the pathophysiology of injury in children different from that in adults. [6, 10]

The neck consists of seven bones, or the cervical vertebrae, which support the head and connect it the body. A cervical fracture is commonly referred to as a broken neck. Cervical spine fractures often occur due to trauma or injury, such as from automobile accidents or slip-and-fall accidents. Imaging diagnostics have advanced to be able to help healthcare professionals diagnose cervical spine health issues.
Dr. Alex Jimenez D.C., C.C.S.T.
Evaluation of injury
When a cervical spine injury is suspected, neck movement should be minimized during transport to the treating facility. Ideally, the patients should be transported on a backboard with a semirigid collar, with the neck stabilized on the sides of the head with sandbags or foam blocks taped from side to side (of the board), across the forehead.
If spinal malalignment is identified, place the patient in skeletal traction with tongs as soon as possible (with very few exceptions), even if no evidence of neurologic deficit exists. The specific injury involved and capabilities of the consulting staff guide further management.
Place tongs one finger width above the earlobes in alignment with the external auditory canal. The consultant applies the tongs for traction under close neurologic and radiograph surveillance. Care must be taken while managing the airway in patients with potential cervical spine injuries. Video-assisted intubation should be considered to limit cervical spine motion during the process of securing the airway. [11, 12, 13, 1]
Cervical spine injuries are best classified according to several mechanisms of injury. These include flexion, flexion-rotation, extension, extension-rotation, vertical compression, lateral flexion, and imprecisely understood mechanisms that may result in odontoid fractures and atlanto-occipital dislocation. [1, 14, 4, 5, 15, 7, 16]
Radiographic evaluation is indicated in the following:
[2, 2, 17, 18, 15, 19, 20]
- Patients who exhibit neurologic deficits consistent with a cord lesion
- Patients with an altered sensorium from head injury or intoxication
- Patients who complain about neck pain or tenderness
- Patients who do not complain about neck pain or tenderness but have significant distracting injuries
A standard trauma series is composed of 5 views: cross-table lateral, swimmer's, oblique, odontoid, and anteroposterior. Approximately 85-90% of cervical spine injuries are evident in the lateral view, making it the most useful view from a clinical standpoint.
The advent of readily available multidetector computed tomography has supplanted the use of plain radiography at many centers. Recent literature supports CT as more sensitive with lower rates of missed primary and secondary injury. [14]
Thoracic Spinal Trauma Imaging
Computed Tomography
Findings
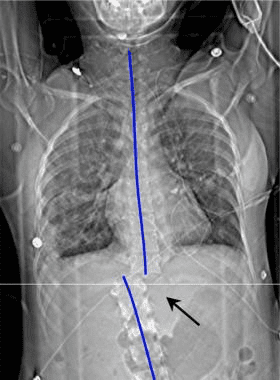
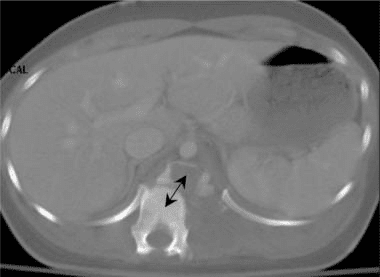
Thin-section axial CT performed by using a bone algorithm is the single most sensitive means by which to diagnose fractures of the thoracic spine. Routine helical CT scans of the thoracic spine are valuable because multisection CT scanners can generate high-resolution spinal images, even during a primary multisystemic trauma evaluation. [21, 22, 28, 29]
The CT images below display various thoracic spinal traumatic injuries.

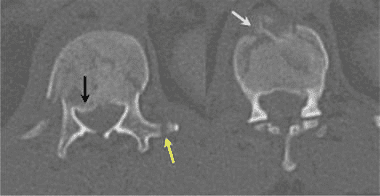
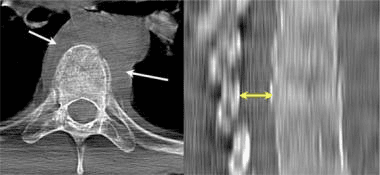
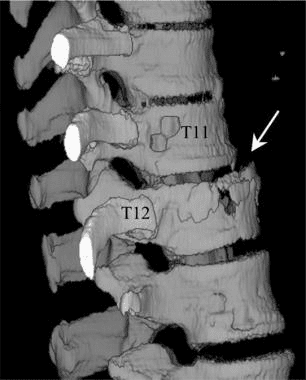
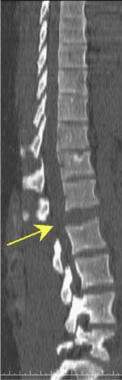
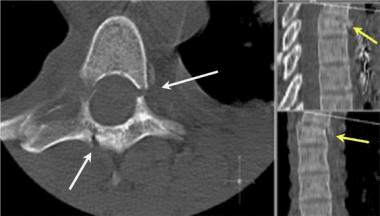
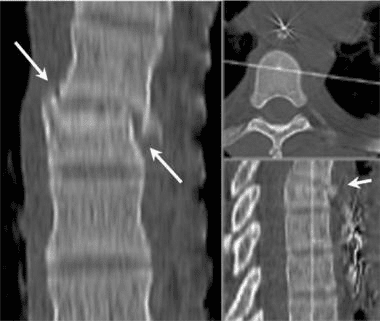

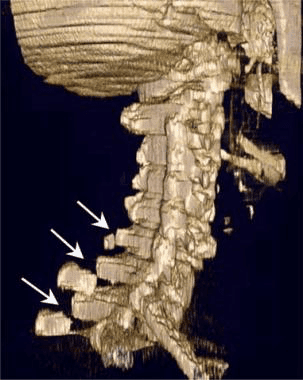
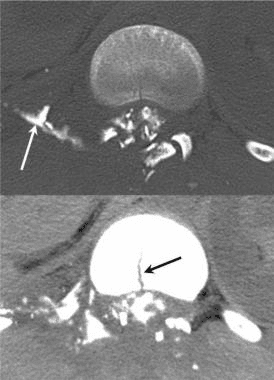
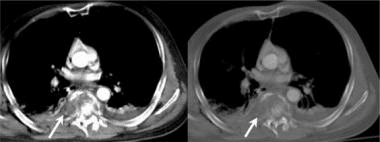
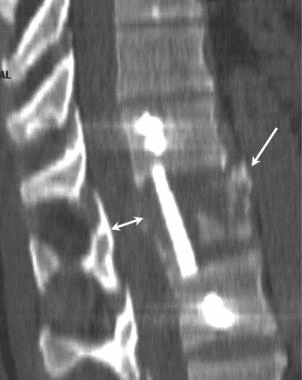
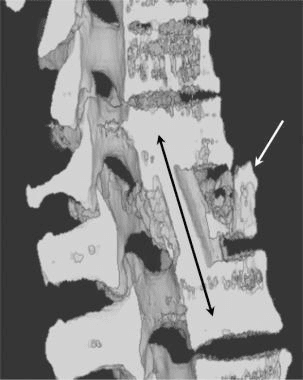
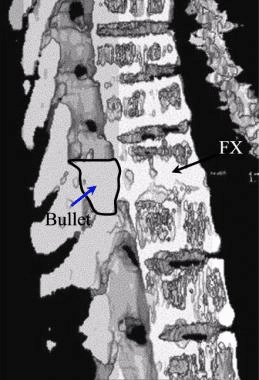
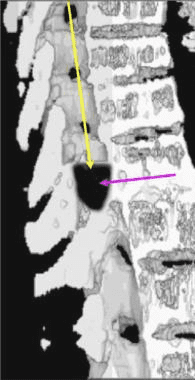
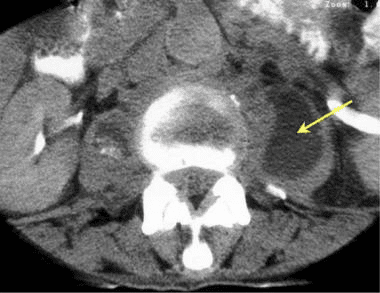
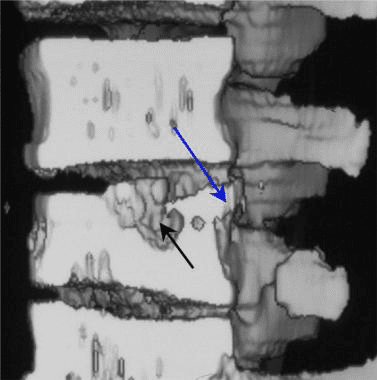
In patients with Chance-type fractures, CT scans often show a burst-type fracture with posterior cortex buckling or retropulsion, and serial transaxial CT images often show a gradual loss of definition of the pedicles. [23]

The thoracic spine, located between the cervical and lumbar vertebrae, consists of 12 vertebrae levels. Thoracic spinal trauma, including spinal cord injuries along the middle of the spine, can generally be severe, however, with early treatment, long-term prognosis is good. Therefore, imaging diagnostics for thoracic spinal trauma are essential. Many healthcare professionals can provide patients with these services.
Dr. Alex Jimenez D.C., C.C.S.T.
Degree of Confidence
The confidence level for the diagnosis of a thoracic spinal fracture with 2-mm axial sections (possible with a multisection CT unit) is greater than 98% and reportedly 99%.
Because axial CT is performed with the patient in a neutral position, a bony distraction of the fracture fragments and subluxations of the spinal articulations may not be as significant on CT images as on acute trauma-series radiographs.
False Positives/Negatives
False-positive results may occur in patients with a Schmorl node, which is a chronic internal herniation of the vertebral disk into the thoracic vertebral body endplate and failure of the fusion of the anterior vertebral endplate epiphysis, resulting in a limbus vertebra. False-negative CT studies may occur in chronic stress injuries and severe generalized osteoporotic endplate fractures.
It has been reported that among trauma patients who had a chest and/or abdominal CT, fractures of the thoracic spine are frequently underreported. Sagittal reformats of the spine obtained from thin sections, and morphometric analysis using electronic calipers help to identify fractures that might otherwise not be identified. [25]
In conclusion, imaging diagnostics of spinal trauma or spine fracture are essential towards the assessment and treatment of patients. Magnetic resonance imaging, or MRI, is helpful in the evaluation of spinal cord and soft-tissue injuries whereas computed tomography scanning, or CT scans, is helpful in the evaluation of spinal trauma or spine fracture. The understanding of imaging technology has tremendously enhanced advances in treatment. The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez

Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.

