




Imaging Diagnosis Management:
- Cervical spinal trauma & radiographic variants simulating disease
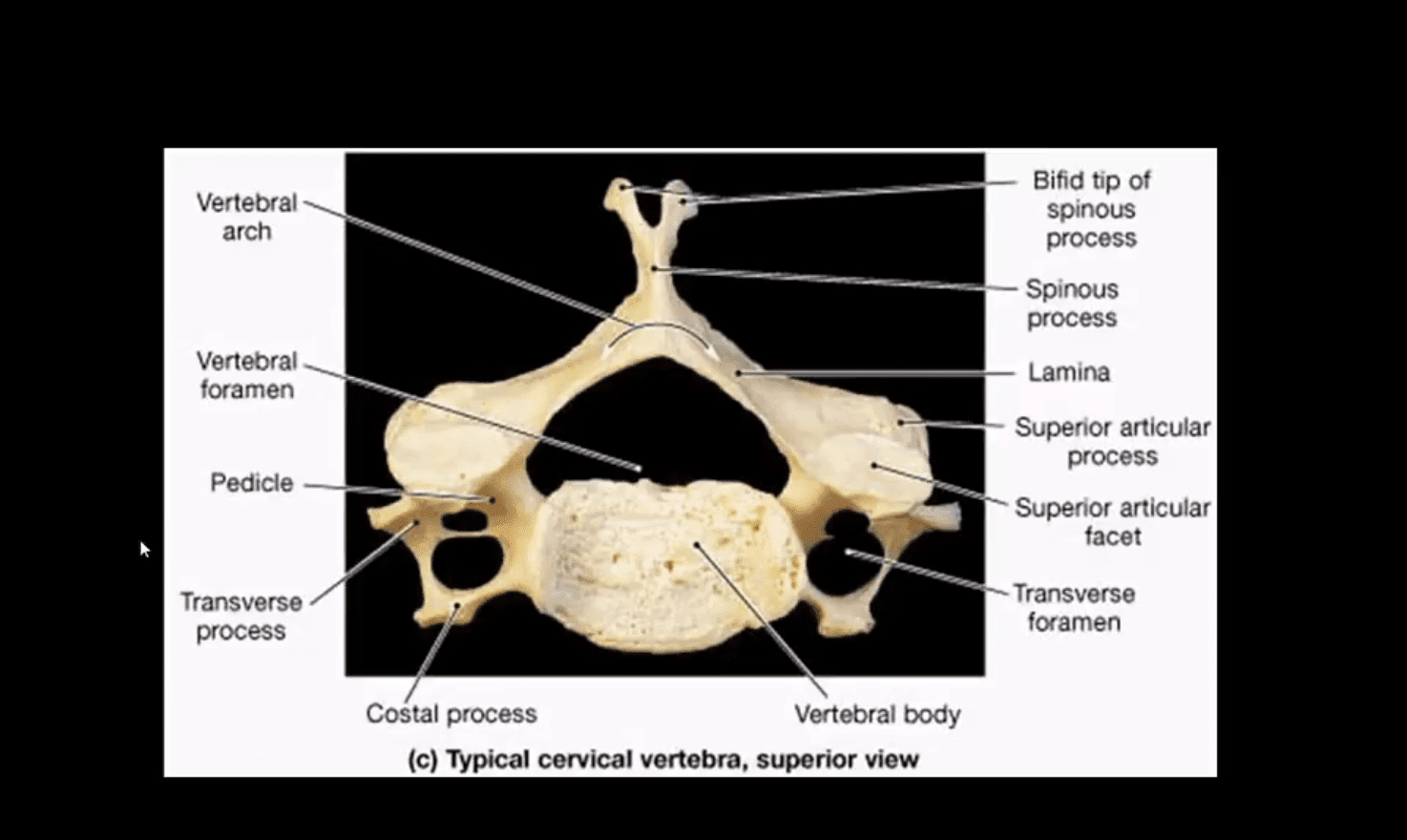
- Cervical spine
- Arthritis
- Neoplasms
- Infection
- Post-Surgical cervical spine
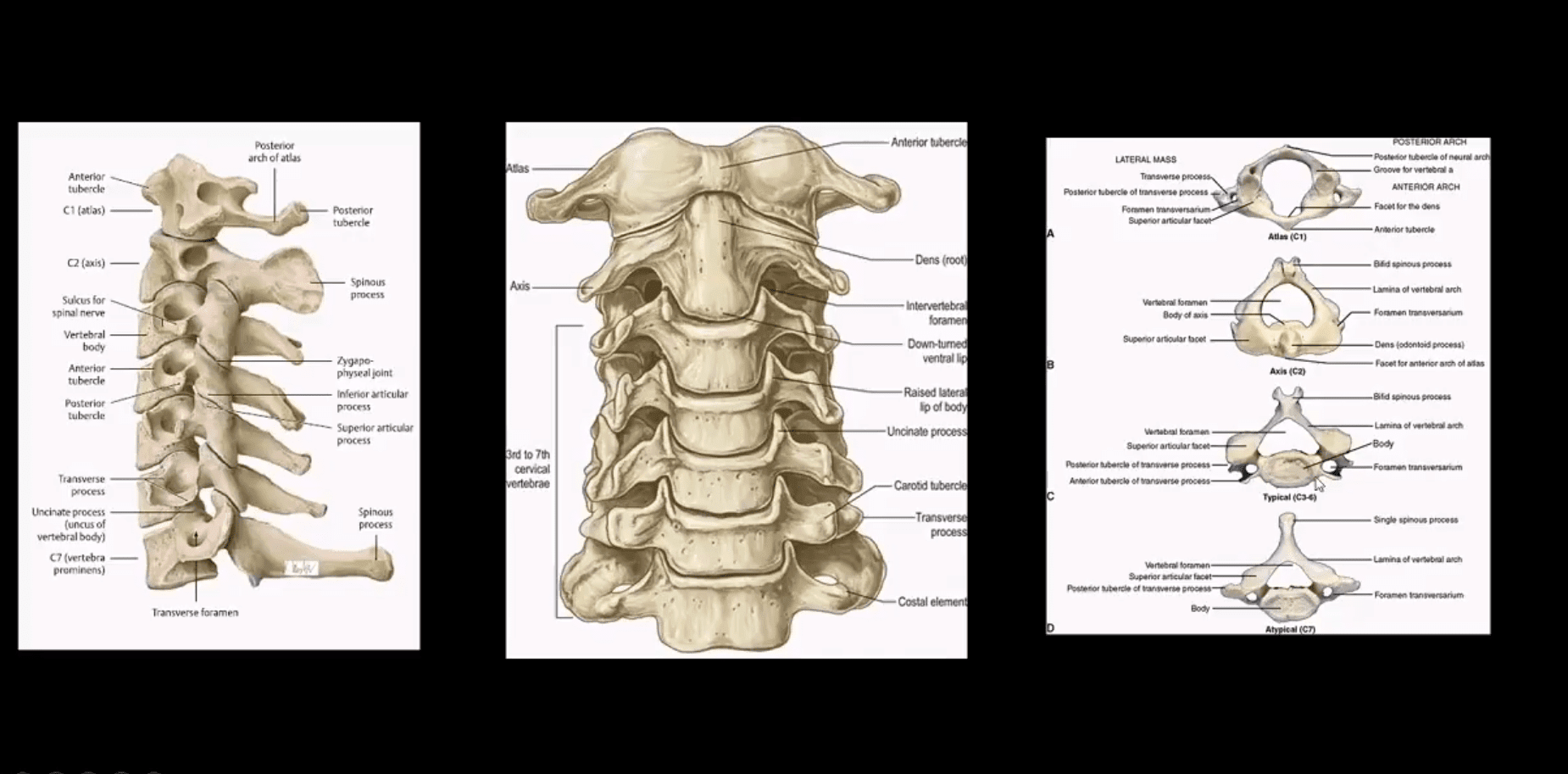
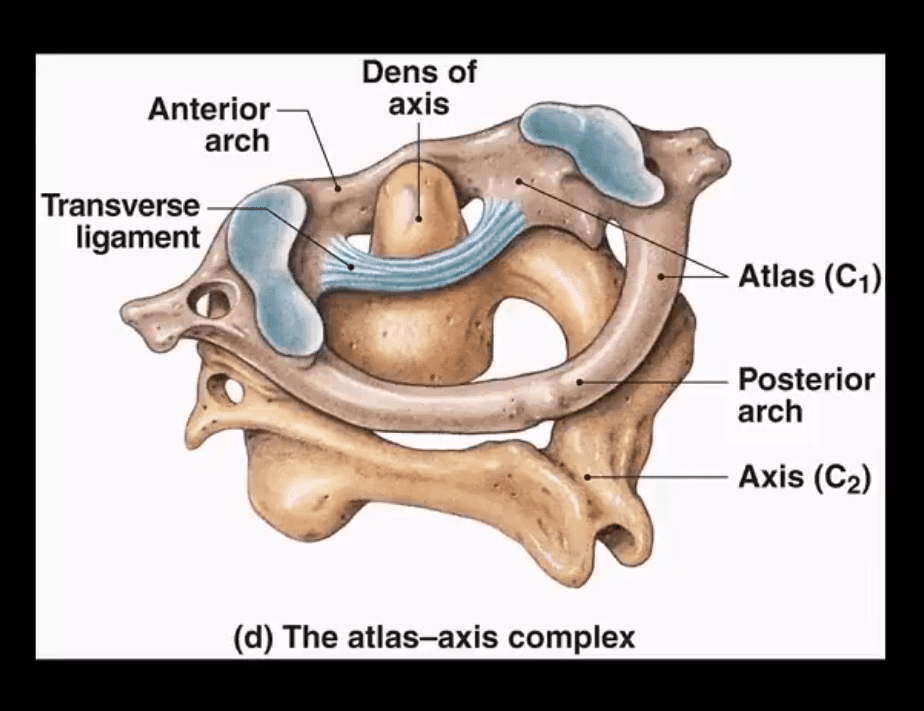
- Cranio-cervical and upper cervical stability is dependent on transverse, superior and inferior bands of the C1-C2 ligament, alar ligaments, along with a few other ligaments
Cervical Trauma
- The C/S is vulnerable to injury. Why?
- Stability has been sacrificed for greater mobility
- Cervical vertebrae are small and interrupted by multiple foraminae
- The head is disproportionately heavy and acts as an abnormal lever especially when forces act against a rigid torso
- Additionally, C/S is prone to degeneration which makes it more vulnerable to trauma
- In young children, ligaments are more luxed vs. disproportionately large head size
- In children, the fulcrum of movement is at C2/3 thus making injuries more common in the upper C/S and craniocervical junction. In children, S.C.I.W.O.R.A. may occur when no evidence of fracture present
- In adults, the fulcrum of movement is at C5/6 thus making lower C/S more vulnerable to trauma especially during extremes of flexion
- Cervical Trauma categorized according to mechanisms of injury (Harris & Mirvis classification)
Hyperflexion Injury: Stable vs. Unstable
- Flexion teardrop Fx (most severe fracture, unstable)
- Bilateral facet dislocation (severe injury w/o fracture, unstable)
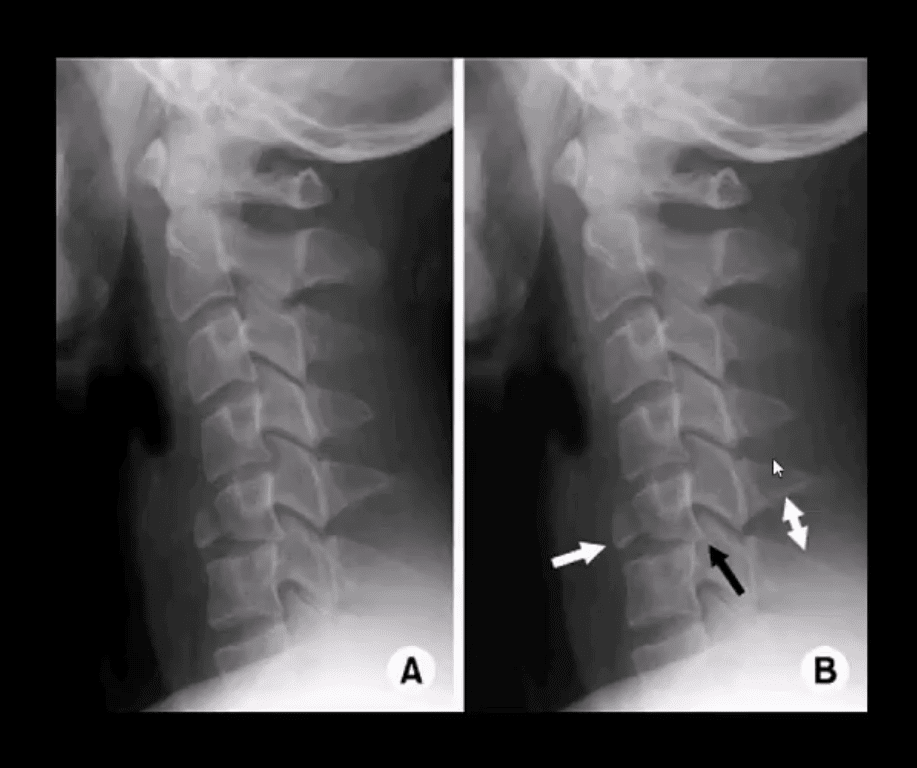
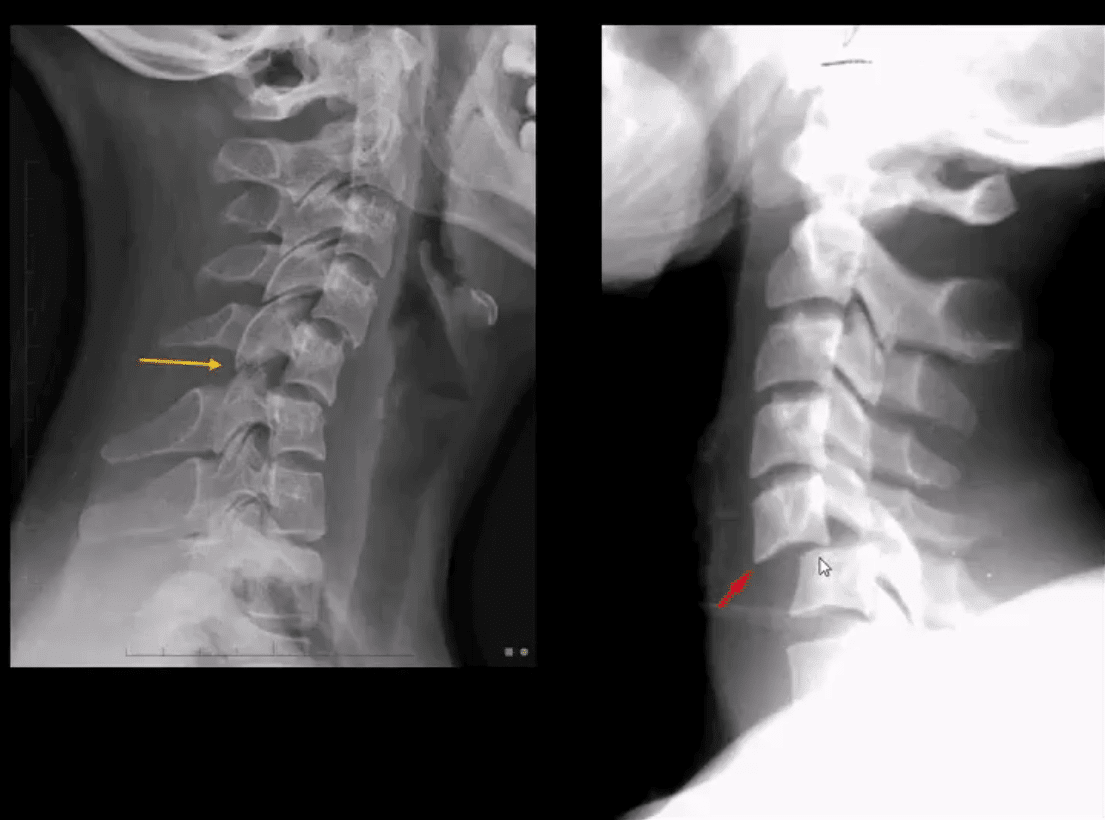
- Anterior subluxation (potentially unstable) can be very subtle injury
- Clay Shoveller Fx (lower C/S SP avulsion, stable)
- Simple wedge compression (most benign Fx, stable)
- Hyperflexion-rotation with unilateral facet dislocation
- Obtain a thorough history
- Perform physical exam including a neurological exam
- Consider NEXUS criteria (National Emergency X-radiography Utilization Study)
Imaging Techniques:
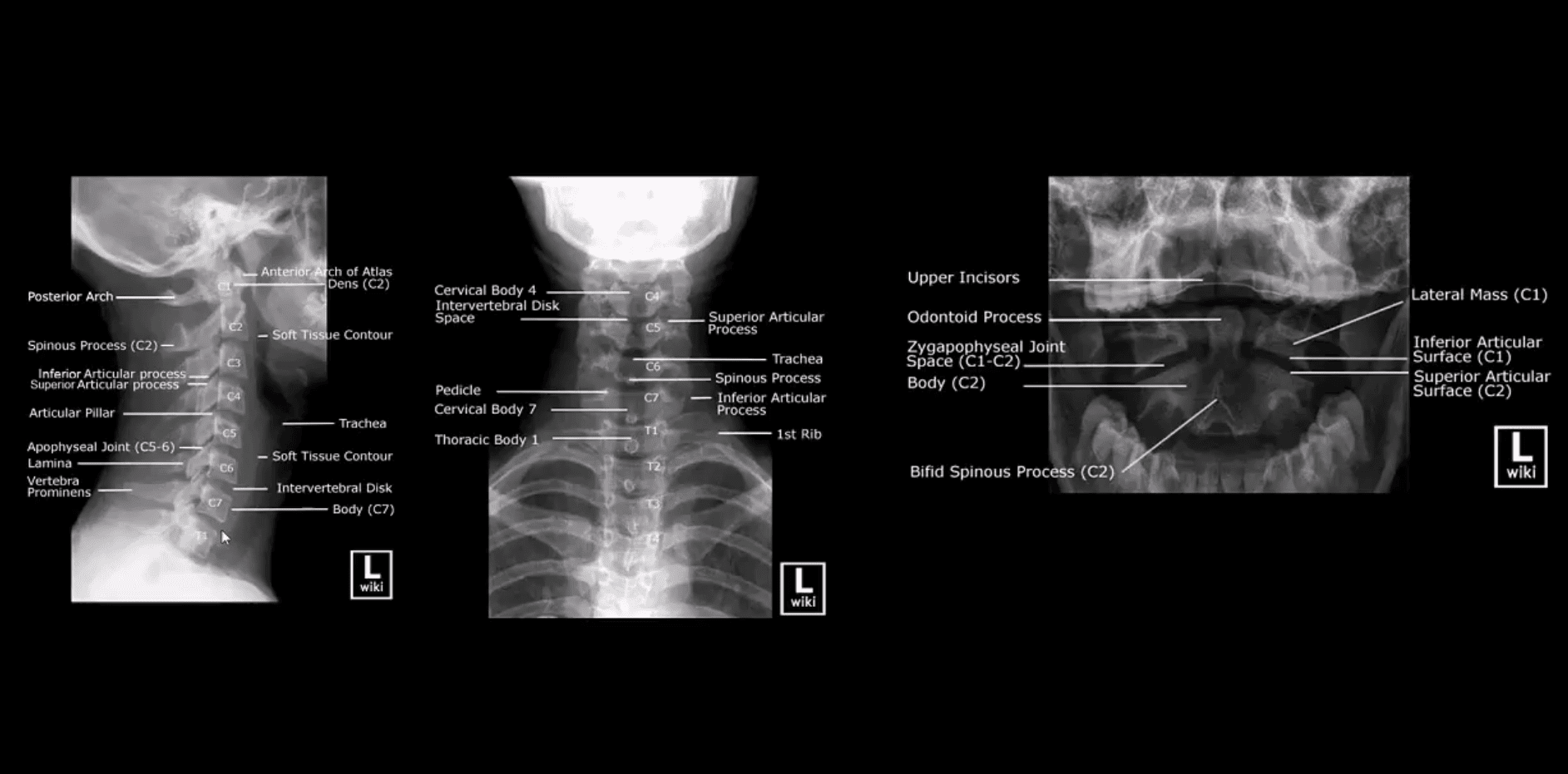
- Begins with x-radiography especially in cases with no significant neurological compromise
- Clear neutral lateral view first
- If x-radiography is unrewarding but high probability of severe trauma and neurological deficit present, CT scanning w/o contrast is required
- Consider CT scanning in patients with pre-existing changes: advance spondylosis, DISH, AS, RA, post-surgical spine, congenital abnormalities (Klippel-Feil syndrome, etc.)
Vertical compression:
- Jefferson aka burst Atlas Fx (unstable especially if the Transverse ligament is torn, cord paralysis in 20-30% only)
- Why? Due to fragments dissociation and canal widening
- Burst Fx of the Thoracic or Lumbar spine (unstable, cord paralysis may occur)
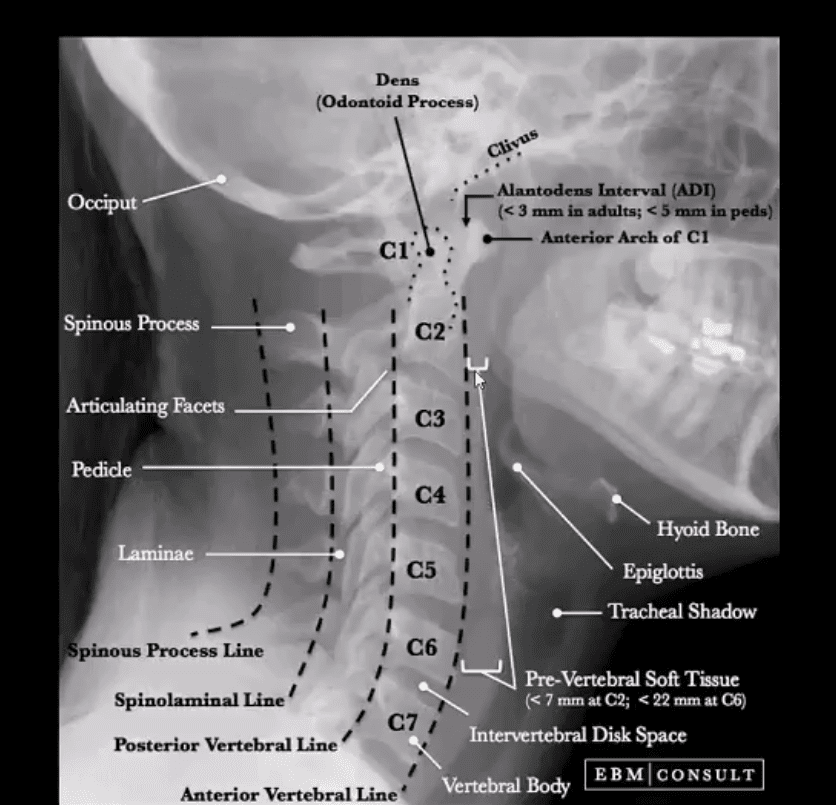
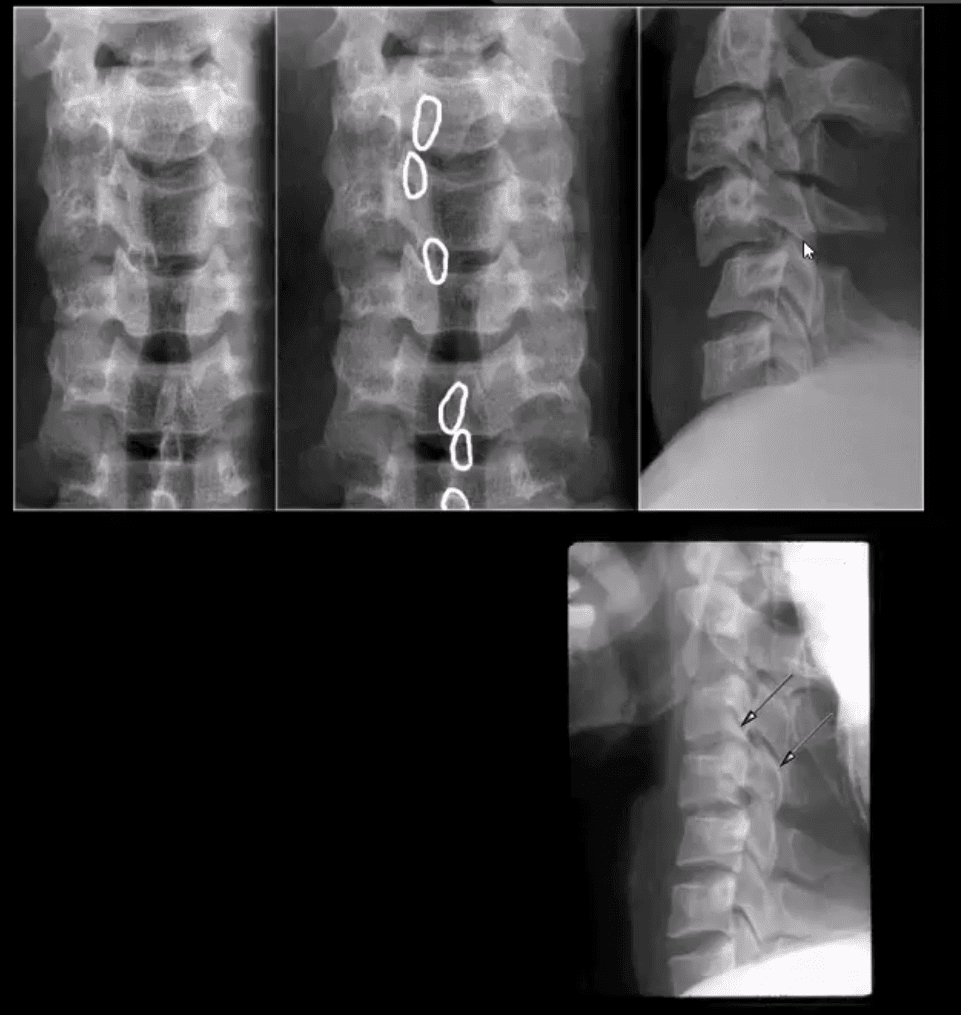
How to Assess Spinal Radiographs in Trauma Cases:
- Construct 5-lines on the lateral view
- Note if facets are well-aligned and symmetrical
- Ensure symmetry of the disc height
- Note any widening or fanning of the inter-spinous distance
- Carefully examine prevertebral soft tissues
- Evaluate atlanto-dental interval (ADI)
- In cases of trauma, evaluate and clear neutral lateral first
- Do not perform flexed and extended views in acute cases before x-rays or CT scanning exclude significant instability
- Pay extra attention to prevertebral soft tissues
- If thicker than normal limits, consider severe post-traumatic bleed
- Subtle asymmetry and widening of posterior disc height and facets with inter-spinous fanning may be a key feature of significant tearing of posterior ligaments
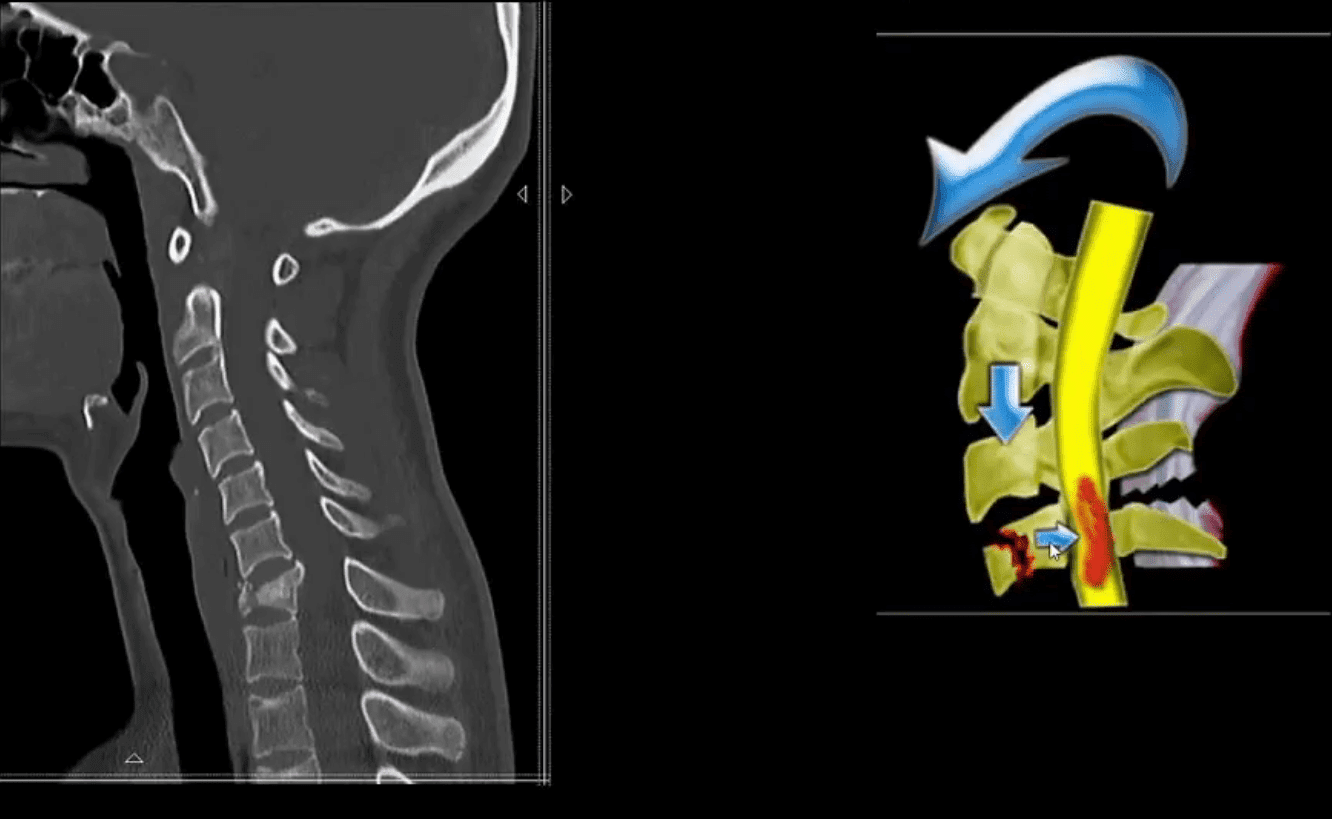
Hyperflexion Injuries (M/C Mechanism)
- More frequent in sub-axial C/S C-3-C7)
- Unstable injuries:
- Flexion teardrop fracture (M/C C5 & C6) v. unstable
- Key rad features:
- Large "teardrop" triangular anterior body fragment
- Fanning of the SPs, posterior disc and facet widening indicating tearing of major spinal ligaments and instability
- A posterior shift of the vertebral body fracture suggests direct anterior cord/vessels compression
- Bulging prevertebral soft tissue >20-mm at C6-7
- 80% of cases may be paralyzed on the spot or develop significant paralysis soon after
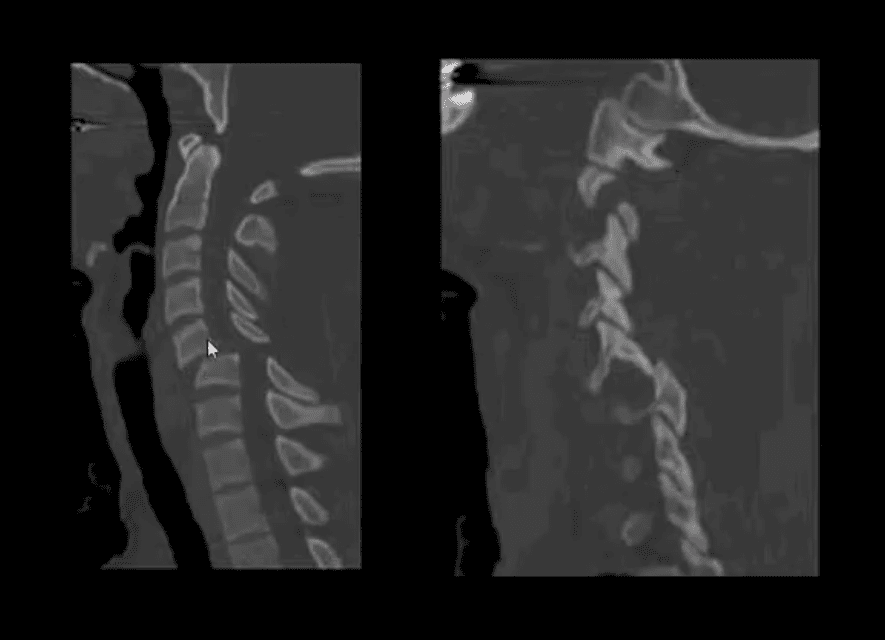
Acute Neck Trauma. What are the vital radiographic features? What is the diagnosis?
- CT scanning w/o contrasts with sagittal reconstruction. Note C7 Flexion teardrop Fx.
- CT may help with further delineation and preoperative planning
- May follow with MR imaging and evaluation of the neurological injury
- Fluid sensitive (T2) sagittal MRI slice of Flexion teardrop fracture at C4 and possibly C5
- Note high signal intensity lesion in the cord and surrounding ligaments indicating cord edema and ischemia
- Management: neurosurgical with spinal fusion
- Complications:
- Quadriplegia/paraplegia
- Respiratory complications
- Disability, changes in the quality of life
- Decreased life expectancy

- Bilateral facet dislocation (unstable)
- Mechanism: Flexion-distraction injury
- Key radiography: anteriorly displaced body 50% or more
- Facets override and locked (can be perched left image)
- Major tearing of ligaments
- Chances of severe cord compression and paralysis
- Patients with ligaments laxity and degenerative changes are at higher risk
- Initial x-radiography is the first step
CT scanning w/o Contrast is Crucial:
- Further delineation of this injury
- Facet fractures, pedicle fracture
- Management planning
Sagittal fluid sensitive MRI of bilateral C5 facet dislocation, sizeable ischemic cord injury, and posterior soft tissue injuries

- Management:
- X-radiography, then CT scanning then immediate closed reduction (esp. if the patient is conscious)
- Followed in some more complicated cases by MRI and then surgical care
- If the patient is awake and neurologically stable, CT and closed reduction are adequate
- Complicated cases and failed closed reduction may require surgical stabilization
- Complications: spinal cord injury and paralysis
- Delayed ligamentous laxity and instability
- Unilateral facet dislocation (flexion-rotation injury) less severe than bilateral dislocation
- Most commonly missed unstable cervical injury on x-radiography
- Key rad features: body anteriorly translated 25% facets appear misaligned and blurred, SPs rotated on frontal views
- Clinically may be presented as one-sided radiculopathy esp. C6 or C7
- CT scanning is required to evaluate further facet/pedicle fractures
- Pre-reduction evaluation and care planning
- Management: closed reduction esp. in a conscious patient
- Complications: acute disc herniation/retropulsion, ligamentous laxity, neurological injury
- https://emedicine.medscape.com/article/824380-overview
- https://emedicine.medscape.com/article/248236-overview#a9
- https://emedicine.medscape.com/article/397896-overview#a3
- https://www.aafp.org/afp/1999/p331.html
