




Neuropathy
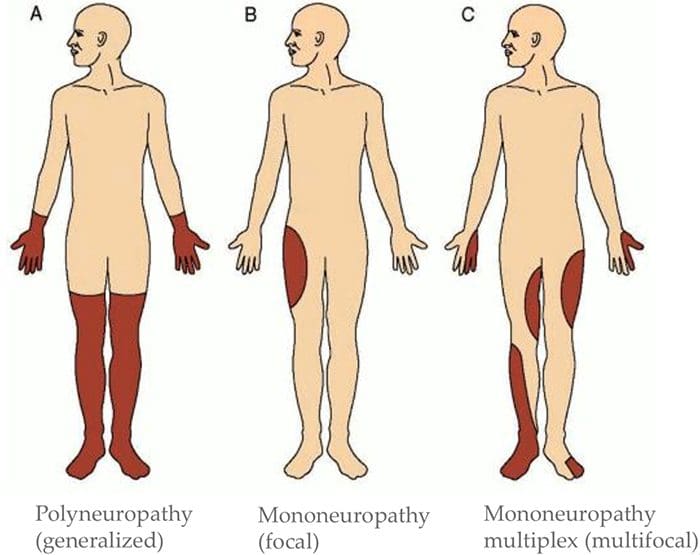
Three primary classifications based on location of symptoms:- Mononeuropathy (focal)
- Mononeuropathy multiplex (multifocal)
- Polyneuropathy (generalized)
- Can involve CNS and/or PNS
- Can affect large and/or small diameter fibers
- Can affect both sensory and motor fibers
- Sometimes one more than the other, but often both
- May be permanent or reversible
Assessment Of Neuropathy
Sensory Exam:
Determine What Sensory Modalities Are Involved
- If sensory disruption is limited to certain modalities, it implies CNS is involved
- If all sensation is affected in the area, implies PNS is involved
Determine Pattern Of Symptoms
- Mononeuropathy (focal)?
- Mononeuropathy multiplex (multifocal)?
- Polyneuropathy (generalized)?
Motor Exam
- Determine if there is change to muscle strength
- Determine if there is a change in muscle tone
- Determine which muscles are affected
- Determine if there has been a change in reflexes
- This information can help determine the level(s) of involvement
Check For Autonomic Signs
- Auscultate heart
- Palpate palms
- Auscultate abdomen
- Assess autonomic history
- For example, is patient complaining about sweating more on one side than another? Complaining of stress levels?
- Suggest ANS involvement
Exams: Merck Manual Professional Version
How To Test Reflexes
How To Do The Sensory Exam
How To Do The Motor Examination
Classification Of Nerve Injuries Resulting In Neuropathy
- Neurapraxia - This is a transient episode of motor paralysis with little or no sensory or autonomic dysfunction; no disruption of the nerve or its sheath occurs; with removal of the compressing force, recovery should be complete
- Axonotmesis - This is a more severe nerve injury, in which the axon is disrupted but the Schwann sheath is maintained; motor, sensory, and autonomic paralysis results; recovery can occur if the compressing force is removed in a timely fashion and if the axon regenerates
- Neurotmesis - This is the most serious injury, in which both the nerve and its sheath are disrupted; although recovery may occur, it is always incomplete, secondary to loss of nerve continuity
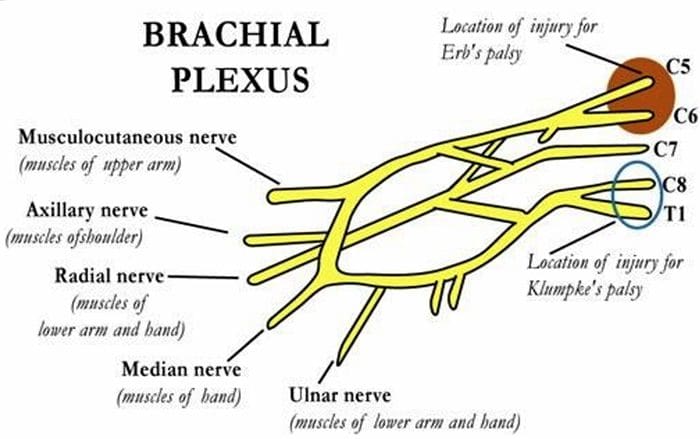
Brachial Plexopathies
- Erb’s Palsy
- Klumke’s Palsy
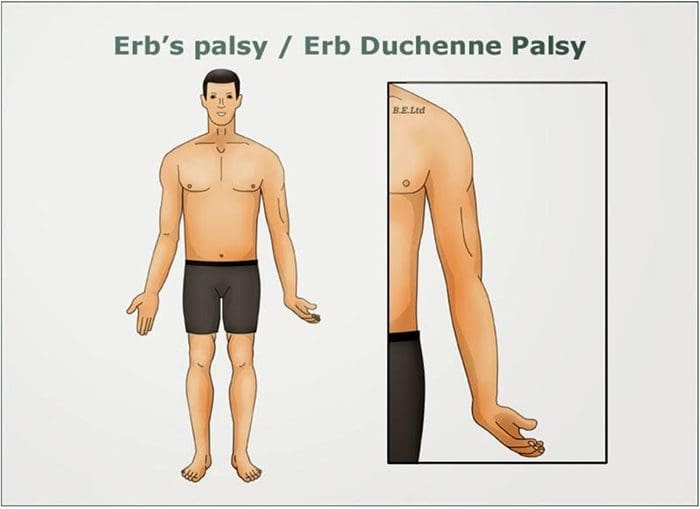
Erb’s Palsy
- AKA Erb–Duchenne palsy or Waiter's tip palsy
- Most common mechanism of injury in adults is a patient who fall forward while holding onto something behind them
- Can also happen to an infant during childbirth Results from damage to C5-6 nerve roots in the brachial plexus
- Dermatomal distribution of sensory disruption
- Weakness or paralysis in deltoid, biceps, and brachialis muscles resulting in “waiter’s tip” position
Klumke’s Palsy
- AKA Dejerine–Klumpke palsy
- Happens to infants during childbirth if arm is pulled overhead
- Can also happen to adults with overhead traction injuries
- Results from damage to C8-T1 nerve roots in the brachial plexus
- Dermatomal distribution of sensory disruption
- Weakness or paralysis in wrist flexors and pronators as well as muscles of the hand
- May produce Horner’s syndrome due to T1 involvement
- Results in a “claw hand” appearance
- Forearm supinated with wrist hyperextended, with finger flexion

Entrapment Neuropathies
- Thoracic Outlet Syndromes
- Median Nerve Entrapment
- Pronator Teres syndrome
- Carpal Tunnel syndrome
- Ulnar Nerve Entrapment
- Cubital Tunnel syndrome
- Tunnel of Guyon syndrome
- Radial Nerve Entrapment
- Spiral Groove Entrapment
- Supinator Syndrome
- Posterior Interosseous Syndrome (Radial Tunnel Syndrome)
- Sciatic Nerve Entrapment
- Piriformis syndrome
- Fibular head entrapment
- Tarsal tunnel syndrome
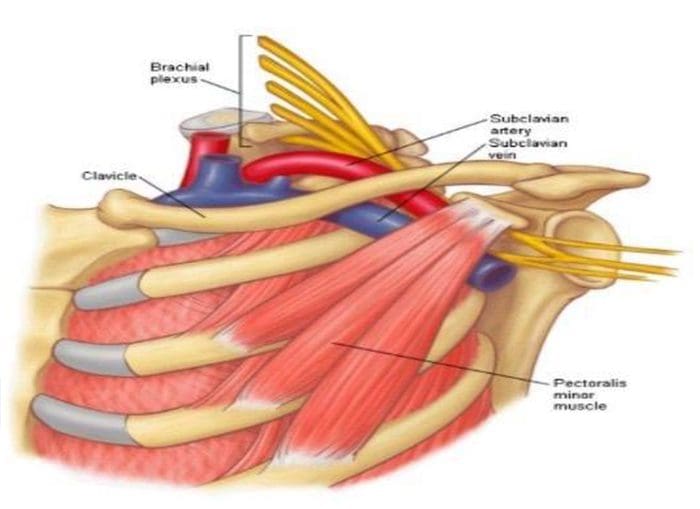
Thoracic Outlet Syndromes

Neurogenic thoracic outlet syndrome
- Compression of the brachial plexus
Vascular thoracic outlet syndrome
- Veins (venous thoracic outlet syndrome) or arteries (arterial thoracic outlet syndrome) are compressed
Nonspecific-type thoracic outlet syndrome
- Worsens with activity
- Idiopathic
Causes
- Cervical rib
- Subclavius muscle tension
- Postural - excessive thoracic kyphosis
- Trauma
- Repetitive activity
- Obesity
- Pregnancy
Tests
- Adsons test
- Allen maneuver
- Costoclavicular maneuver
- Halstead maneuver
- Reverse bakody maneuver
- Roos test
- Shoulder compression test
- Wright test
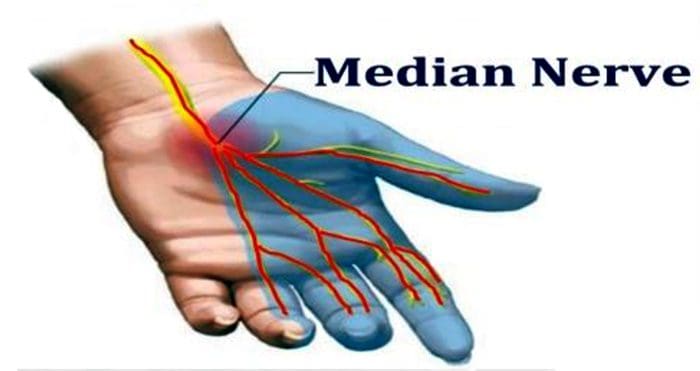
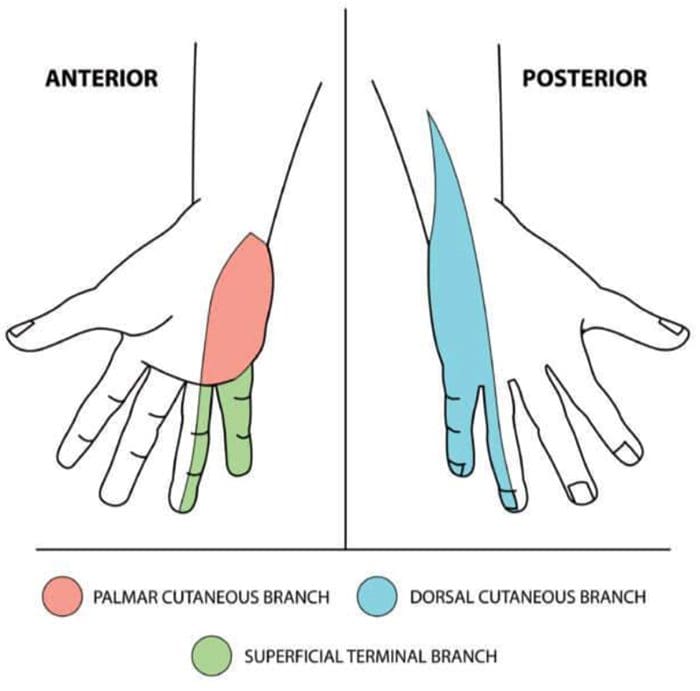
Median Nerve Entrapment
- Sensory disruption in the lateral portion (3.5 fingers) of the palmar aspect of the hand, and dorsal finger tips of the same fingers
- Motor fibers affected in forearm if applicable, muscles of the thenar eminence
- Abductor pollicis brevis
- Opponens pollicis
- Flexor pollicis brevis
Median N. Pronator Teres Syndrome
Etiology
- Compression of the median nerve at the elbow
Causes
- Repetitive movement
- Pronator teres muscle inflammation
- Thickened bicipital aponeurosis
Findings
- Tenderness with palpation of the pronator teres muscle
- Pain with resisted pronation of the arm
- Flexor pollicus longus and flexor digitorum profundus involvement
- Otherwise may appear similar to carpal tunnel syndrome in symptoms, but without positive wrist orthopedics
Median N. Carpal Tunnel Syndrome
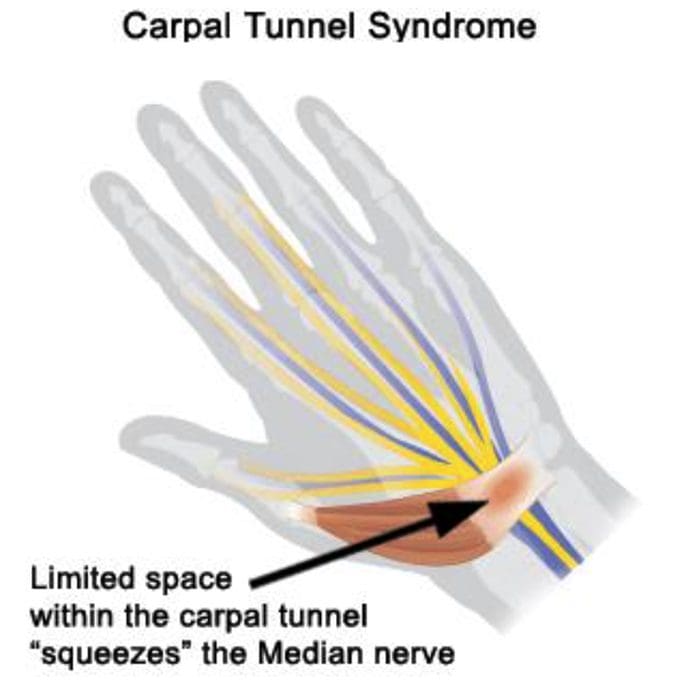
Etiology
- Compression of the median nerve at the wrist
Causes
- Repetitive motions
- Hypothyroidism
- Obesity
- Rheumatoid Arthritis
- Diabetes
- Pregnancy
Orthopedic Tests
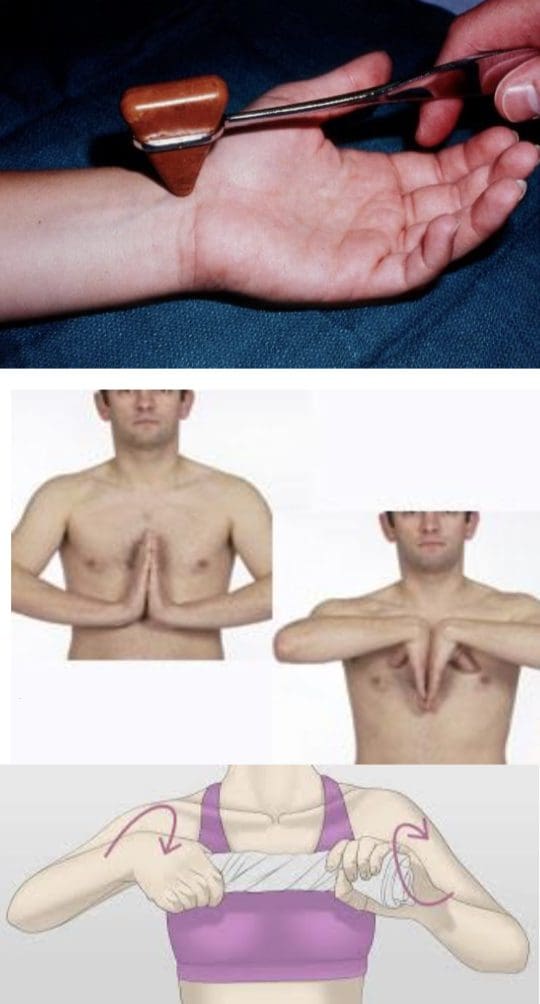
Tinel’s Sign
- Positive if tapping over the median nerve reproduces/exacerbates symptoms
Phalen’s Maneuver/Prayer Sign
- Hands together with wrists flexed
- Repeat in reverse with wrists extended
- Hold each for at least 60 seconds
- Positive if tests reproduce/exacerbate symptoms
Wringing Test
- Wringing a towel produces paresthesia
Ulnar Nerve Entrapment
- Sensory disruption in the medial two digits of the palmar & dorsal aspects of the hand
- Motor fibers affected in hand, all fingers besides the thumb weakened general hand weakness
Ulnar N. Cubital Tunnel Syndrome
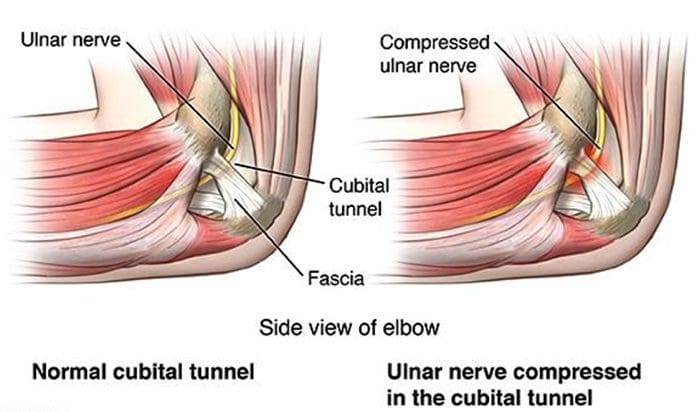
Etiology
- Compression of the ulnar nerve at the elbow
Causes
- Repetitive motions
- Hypothyroidism
- Obesity
- Diabetes
- Trauma to the cubital tunnel
- Prolonged sitting with pressure on bent elbow
Ulnar N. Tunnel Of Guyon Syndrome
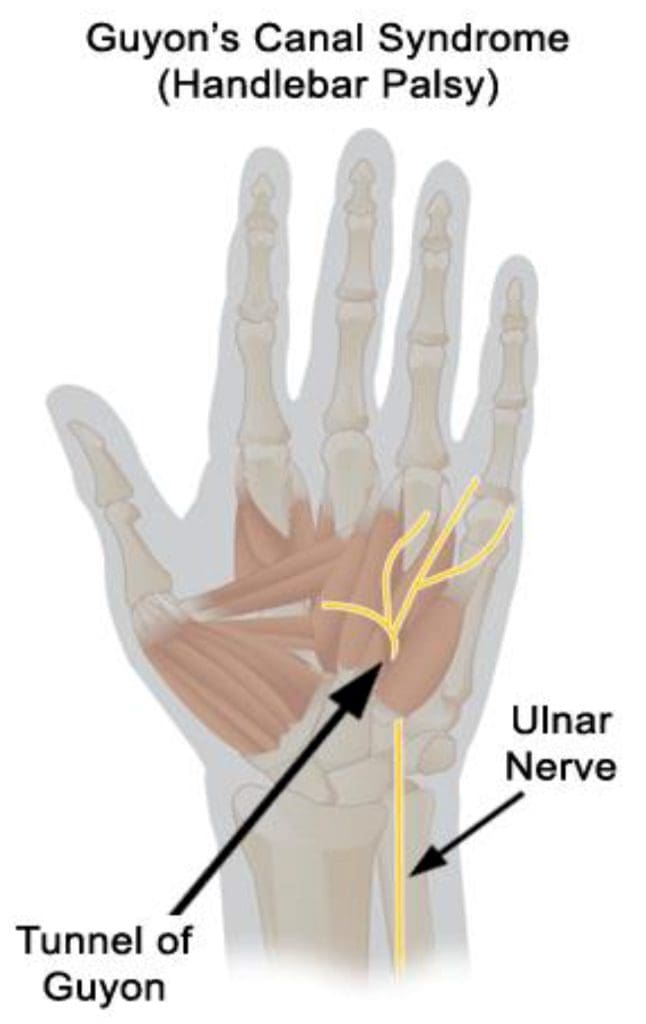
Etiology
- Compression of the ulnar nerve at the wrist
Causes
Repetitive motions- Long term crutch use
- Break of the hamate
- Ganglion cyst
- Hypothyroidism
- Obesity
- RheumatoidArthritis
- Diabetes
Orthopedic Tests
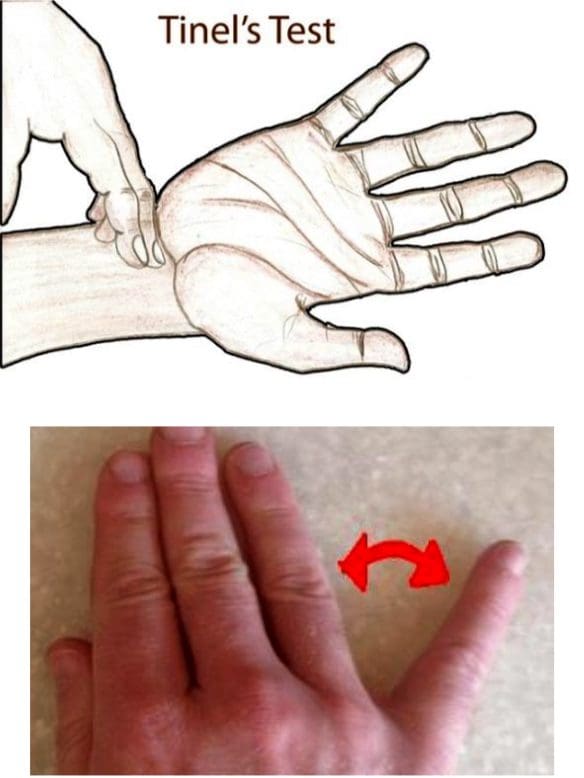
Tinel’s Sign
- Present if test over the ulnar nerve at the wrist elicits symptoms
Wartenberg Sign
- 5th digit abducts when patient performs hard grip strength test or attempts to squeeze fingers together
- Reduced two-point discrimination in the hand
Radial Nerve Entrapment
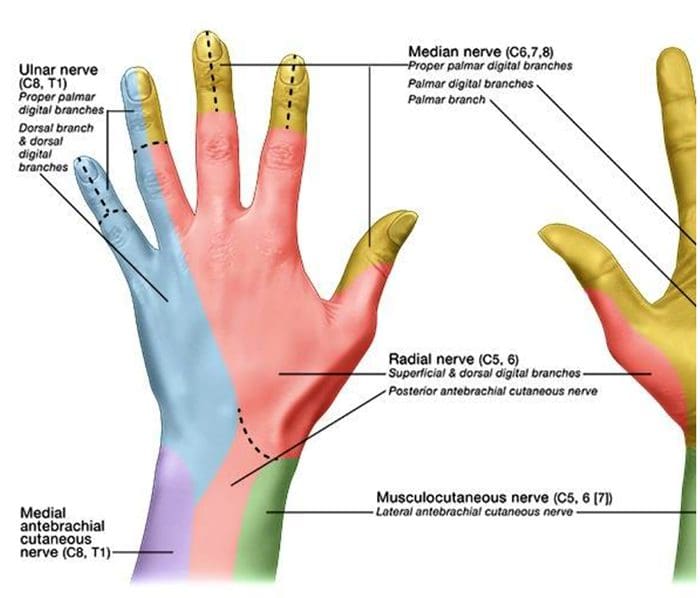
- Sensory disruption in the lateral 3.5 digits of the dorsal aspect of the hand
- Motor fibers affected in posterior arm and extensor compartment of the forearm
- Wrist drop may be seen
Spiral Groove Entrapment
- All radial nerve innervated muscles below entrapment are affected
- “Saturday night palsy” (from sleeping on own arm)
- Brachioradialis & triceps reflexes both diminished
Supinator Syndrome
- Compression at the arcade of Frohse
- No change in reflexes
Posterior Interosseous Syndrome (Radial Tunnel Syndrome)
- No change in reflexes
National University of Health Sciences Master of Science (MS) - Advanced Clinical Practice (ACP) MS ACP 551: Clinical Neurology © 2018
Sources
Blumenfeld, Hal. Neuroanatomy through Clinical Cases. Sinauer, 2002.
Evans, Ronald C. Illustrated Orthopedic Physical Assessment. Mosby/Elsevier, 2009.
“Radial Nerve Entrapment: Background, Anatomy, Pathophysiology.” Medscape, 25 Oct. 2017, emedicine.medscape.com/article/1244110- overview#a8.
