




In the modern world, it's easy to find circumstances to stress about. Whether it involves work, financial issues, health emergencies, relationship problems, media stimulation and/or other factors, stress can begin to weigh in on our overall health and wellness if not managed properly. Also, we often tend to create stress ourselves through poor nutrition and a lack of sleep.
In fact, more than three-fourths of the population in the United States experiences stress on a regular basis, where one-third of those individuals characterize their stress levels as "extreme". Although short-term stress can be helpful, long-term stress can lead to a variety of health issues. Stress has been considered the cause of so many diseases, healthcare professionals estimate it accounts for half of the country's healthcare-related expenses, according to the U.S. News & World Report.
How Stress Affects the Body
Stress signals the sympathetic nervous system to trigger the "fight or flight" response, a defense mechanism which prepares the body for perceived danger by causing the heart rate, blood volume and blood pressure to rise. This diverts blood away from the digestive system and limbs. The adrenal glands also secrete a special mixture of hormones and chemicals, including adrenaline, epinephrine and norepinephrine, which could affect an individual's well-being if they're constantly being secreted into the body.
Also, chronic stress can cause muscle tension. Excess muscle tension along the neck and back may result in the misalignment of the spine, known as a subluxation, ultimately interfering with the proper function of the nervous system and causing symptoms of back pain and sciatica. Fortunately, a variety of stress management techniques, including chiropractic care and mindfulness meditation, can help reduce chronic pain, commonly associated with chronic stress.
Chiropractic Care for Stress
Chiropractic care is a well-known, alternative treatment option utilized to treat a variety of injuries and conditions associated with the musculoskeletal and nervous system. Correcting spinal misalignments is the first step for reducing stress. If there is a subluxation in the spine, the nervous system may often not be able to properly send signals throughout the rest of the body. By using spinal adjustments and manual manipulations, a doctor of chiropractic can carefully realign the spine, releasing muscle tension, soothing irritated spinal nerves and improving blood flow, changes which could will alert the brain to switch off the "fight or flight" response so that the body can return to a more relaxed state.
Furthermore, a chiropractor can also recommend lifestyle modifications, together with spinal adjustments and manual manipulations, to help reduce stress. Nutritional supplementation, rehabilitative exercises, deep-tissue massage, relaxation techniques and posture changes recommended by a chiropractor are several stress management techniques which can help improve symptoms of chronic pain associated with stress. The following article is a systematic review and meta-analysis demonstrating the use of mindfulness medication for chronic pain, including back pain and sciatica.
Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis
Abstract
- Background: Chronic pain patients increasingly seek treatment through mindfulness meditation.
- Purpose: This study aims to synthesize evidence on efficacy and safety of mindfulness meditation interventions for the treatment of chronic pain in adults.
- Method: We conducted a systematic review on randomized controlled trials (RCTs) with meta-analyses using the Hartung-Knapp-Sidik-Jonkman method for random-effects models. Quality of evidence was assessed using the GRADE approach. Outcomes included pain, depression, quality of life, and analgesic use.
- Results: Thirty-eight RCTs met inclusion criteria; seven reported on safety. We found low-quality evidence that mindfulness meditation is associated with a small decrease in pain compared with all types of controls in 30 RCTs. Statistically significant effects were also found for depression symptoms and quality of life.
- Conclusions: While mindfulness meditation improves pain and depression symptoms and quality of life, additional well-designed, rigorous, and large-scale RCTs are needed to decisively provide estimates of the efficacy of mindfulness meditation for chronic pain.
- Electronic supplementary material: The online version of this article (doi:10.1007/s12160-016-9844-2) contains supplementary material, which is available to authorized users.
- Keywords: Chronic pain, Mindfulness, Meditation, Systematic review
Introduction
Chronic pain, often defined as pain lasting longer than 3 months or past the normal time for tissue healing [1], can lead to significant medical, social, and economic consequences, relationship issues, lost productivity, and larger health care costs. The Institute of Medicine recognizes pain as a significant public health problem that costs our nation at least $560–635 billion annually, including costs of health care and lost productivity [2]. Further, chronic pain is frequently accompanied by psychiatric disorders such as pain medication addiction and depression that make treatment complicated [3]. The high prevalence and refractory nature of chronic pain, in conjunction with the negative consequences of pain medication dependence, has led to increased interest in treatment plans that include adjunctive therapy or alternatives to medication [4]. One such modality that pain patients are using is mindfulness meditation. Based on ancient Eastern meditation practices, mindfulness facilitates an attentional stance of detached observation. It is characterized by paying attention to the present moment with openness, curiosity, and acceptance [5, 6]. Mindfulness meditation is thought to work by refocusing the mind on the present and increasing awareness of one’s external surroundings and inner sensations, allowing the individual to step back and reframe experiences. Current research using neuroimaging to elucidate neurological mechanisms underlying effects of mindfulness has focused on brain structures such as the posterior cingulate cortex, which appear to be involved in self-referential processing [7, 8]. Clinical uses of mindfulness include applications in substance abuse [9], tobacco cessation [10], stress reduction [11], and treatment of chronic pain [12–14].
Early mindfulness studies in pain patients showed promising outcomes on pain symptoms, mood disturbance, anxiety, and depression, as well as pain-related drug utilization [5]. Numerous systematic reviews on the effects of mindfulness meditation have been published in recent years. Of those that report pain outcomes, several have focused on specific types of pain such as low back pain [13], fibromyalgia [15], or somatization disorder [16]. Others were not limited to RCTs [14, 17]. There have been several comprehensive reviews focused on controlled trials of mindfulness interventions for chronic pain including a review [4] that showed improvements in depressive symptoms and coping, another review [18] on mindfulness for chronic back pain, fibromyalgia, and musculoskeletal pain that showed small positive effects for pain, and the most recent review [19] on various pain conditions which found improvements in pain, pain acceptance, quality of life, and functional status. Authors of these reviews echoed concerns that there is limited evidence for efficacy of mindfulness-based interventions for patients with chronic pain because of methodological issues. They have concluded that additional high-quality research was needed before a recommendation for the use of mindfulness meditation for chronic pain symptoms could be made.
The purpose of this study was to conduct a systematic review and meta-analysis of the effects and safety of mindfulness meditation, as an adjunctive or monotherapy to treat individuals with chronic pain due to migraine, headache, back pain, osteoarthritis, or neuralgic pain compared with treatment as usual, waitlists, no treatment, or other active treatments. Pain was the primary outcome, and secondary outcomes included depression, quality of life, and analgesic use. The systematic review protocol is registered in an international registry for systematic reviews (PROSPERO 2015:CRD42015025052).
Methods
Search Strategy
We searched the electronic databases PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, and Cochrane Central Register of Controlled Trials (CENTRAL) for English-language-randomized controlled trials from inception through June 2016. We combined pain conditions and design terms with the following mindfulness search terms: “Mindfulness” [Mesh]) or “Meditation” [Mesh] or mindfulness* or mindfulness-based or MBSR or MBCT or M-BCT or meditation or meditat* or Vipassana or satipaṭṭhāna or anapanasati or Zen or Pranayama or Sudarshan or Kriya or zazen or shambhala or buddhis*.” In addition to this search and the reference mining of all included studies identified through it, we reference mined prior systematic reviews and retrieved all studies included therein.
Eligibility Criteria
Parallel group, individual or cluster RCTs of adults who report chronic pain were included. Studies where the author defined chronic pain and studies in patients reporting pain for a minimum of 3 months were included. Studies were required to involve mindfulness meditation, either as an adjunctive or monotherapy; studies testing other meditation interventions such as yoga, tai chi, qigong, and transcendental meditation techniques without reference to mindfulness were excluded. Mindfulness interventions that did not require formal meditation, such as acceptance and commitment therapy (ACT) were also excluded. Only studies that reported pain measures or change in analgesic use were included. Dissertations and conference abstracts were excluded.
Procedures
Two independent reviewers screened titles and abstracts of retrieved citations—following a pilot session to ensure similar interpretation of the inclusion and exclusion criteria. Citations judged as potentially eligible by one or both reviewers were obtained as full text. The full text publications were then dually screened against the specified inclusion criteria. The flow of citations throughout this process was documented in an electronic database, and reasons for exclusion of full-text publications were recorded. Data abstraction was also conducted in dual. Risk of bias was assessed using the Cochrane Risk of Bias tool [20]. Other biases related to the US Preventive Services Task Force’s (USPSTF) criteria for internal validity of included studies were assessed [21, 22]. These criteria were used to rate the quality of evidence as good, fair, or poor for each included study.
Meta-Analytic Techniques
When sufficient data were available and statistical heterogeneity was below agreed thresholds [20], we performed meta-analysis to pool efficacy results across included studies for the outcomes of interest and present a forest plot for the main meta-analysis. We used the Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis using unadjusted means and measures of dispersion [23–25]. For studies reporting multiple pain outcomes, we used specific pain measures, such as the McGill Pain Questionnaire (MPQ) for the main meta-analysis rather than the pain subscale of the SF-36, and average or general pain measures rather than situational measures such as pain at the time of assessment. Due to the small number of adverse events reported, quantitative analysis was not conducted. We conducted subgroup analyses and meta-regressions to address whether there were differences in effect sizes between different interventions types, populations, or when used as monotherapy versus an adjunctive therapy. The quality of the body of evidence was assessed using the GRADE approach [22, 26] by which a determination of high, moderate, low, or very low was made for each major outcome [27].
Results
Description of Included Studies
We identified 744 citations through searches of electronic databases and 11 additional records identified through other sources (see Figure 1). Full texts were obtained for 125 citations identified as potentially eligible by two independent reviewers; 38 RCTs met inclusion criteria. Details of study characteristics are displayed in Table 1 and effects for individual studies are displayed in Table 2.
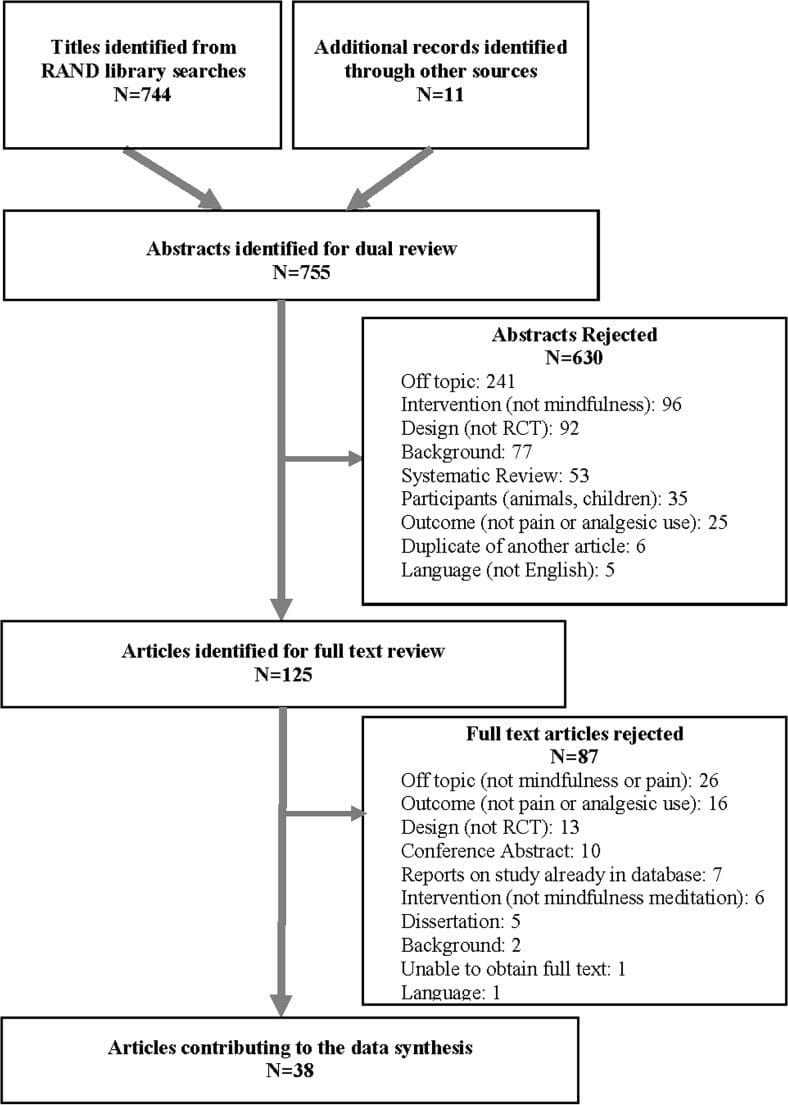
Figure 1: Literature flow diagram.
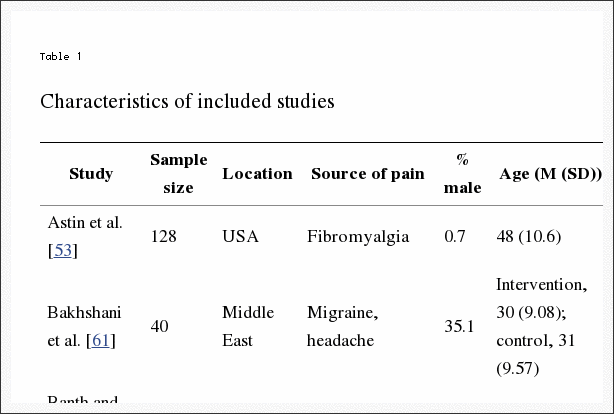
Table 1: Characteristics of included studies.
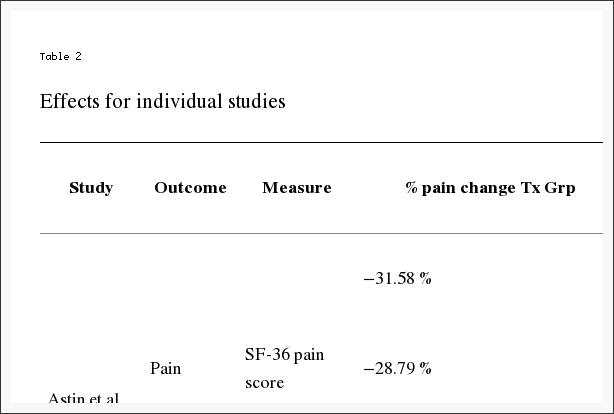
Table 2: Effects for individual studies.
In total, studies assigned 3536 participants; sample sizes ranged from 19 to 342. Fifteen studies reported an a priori power calculation with targeted sample size achieved, ten studies did not report information about a power calculation, and three studies were unclear in the reporting of a power calculation. Ten studies noted there was insufficient power; the authors considered these pilot studies. The majority of the studies were conducted in North America or Europe. The mean age of participants ranged from 30 (SD, 9.08) to 78 years (SD, 7.1. Eight studies included only female participants.
Medical conditions reported included fibromyalgia in eight studies and back pain in eight studies. (Categories are not mutually exclusive; some studies included patients with different conditions.) Osteoarthritis was reported in two studies and rheumatoid arthritis in three. Migraine headache was reported in three studies and another type of headache in five studies. Three studies reported irritable bowel syndrome (IBS). Eight studies reported other causes of pain and three studies did not specify a medical condition or source of chronic pain.
The total length of the interventions ranged from 3 to 12 weeks; the majority of interventions (29 studies) were 8 weeks in length. Twenty-one studies were conducted on mindfulness-based stress reduction (MBSR) and six on mindfulness-based cognitive therapy (MBCT). Eleven additional studies reported results on other types of mindfulness training. Thirteen RCTs provided the mindfulness intervention as monotherapy, and eighteen utilized a mindfulness intervention as adjunctive therapy, specifying that all participants received this in addition to other treatment such as medication. Seven of the studies were unclear as to whether the mindfulness intervention was monotherapy or adjunctive therapy. Nineteen RCTs used treatment as usual as comparators, thirteen used passive comparators, and ten used education/support groups as comparators. Beyond these common comparators, one study each used stress management, massage, a multidisciplinary pain intervention, relaxation/stretching, and nutritional information/food diaries as comparators; two studies used cognitive-behavioral therapy. Several studies had two comparison arms.
Study Quality and Risk of Bias
The study quality for each included study is displayed in Table 1. Eleven studies obtained a “good” quality rating [28–38]. Fourteen studies were judged to be of fair quality, primarily due to being unclear in some aspects of the methods [39–52]. Thirteen studies were judged to be poor; ten primarily due to issues with completeness of reporting outcome data such as inadequate or missing intention to treat (ITT) analysis and/or less than 80 % follow-up [53–62] and three due to unclear methods [63–65]. Details of the quality ratings and risk of bias for each included study is displayed in Electronic Supplementary Material 1.
Measures
Studies reported patient pain measures such as the Visual Analog Scale, the SF-36 pain subscale, and McGill Pain Questionnaire. Secondary outcome measures included depression symptoms (e.g., Beck Depression Inventory, Patient Health Questionnaire), physical and mental health-related quality of life (e.g., SF-36 mental and physical components), and functional impairment/disability (e.g., Roland-Morris Disability Questionnaire, Sheehan Disability Scale).
Chronic Pain Treatment Response
Thirty RCTs reported continuous outcome data on scales assessing chronic pain [29, 31–33, 36, 39–49, 51–60, 62–64, 66].
Eight studies met screening inclusion criteria but did not contribute to the meta-analysis because they did not report poolable data [28, 30, 34, 35, 38, 50, 61, 65]. Their study characteristics are displayed in Table 1, and study level effects along with the reasons they were not in pooled analyses are displayed in Table 2.
Pain scales and comparators varied from study to study. The median follow-up time was 12 weeks, with a range of 4 to 60 weeks. Figure 2 displays the results of meta-analysis using data at the longest follow-up for each study. The pooled analysis indicates a statistically significant effect of mindfulness meditation compared with treatment as usual, passive controls, and education/support groups (SMD, 0.32; 95 % CI, 0.09, 0.54; 30 RCTs). Substantial heterogeneity was detected (I 2 = 77.6 %). There was no evidence of publication bias (Begg’s p = 0.26; Egger’s test p = 0.09). To investigate whether the treatment estimate is robust when excluding poor-quality studies and to explore the possible source of the substantial heterogeneity, we conducted a sensitivity analysis including only fair or good quality studies. The improvement remained significant, the effect size was smaller (SMD, 0.19; 95 % CI, 0.03, 0.34; 19 RCTs), and there was less heterogeneity (I 2 = 50.5 %). Meta-regressions showed that changes in pain outcomes in good- (p = 0.42) and fair-quality (p = 0.13) studies were not significantly different from changes in poor-quality studies.
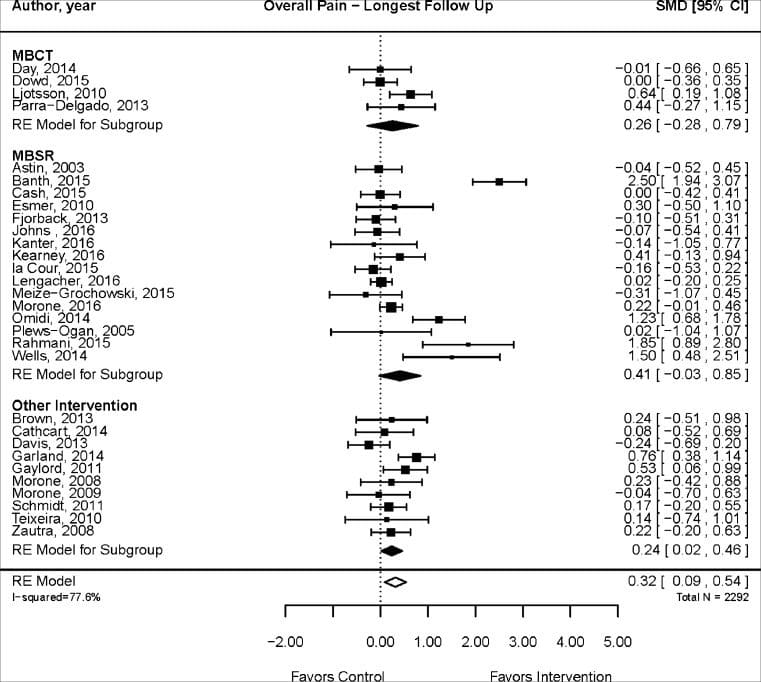
Figure 2: Mindfulness meditation effects on chronic pain.
In subgroup analyses, the effect was not statistically significant at 12 weeks or less (SMD, 0.25; 95 % CI, −0.13, 0.63; 15 RCTs; I 2 = 82.6 %) but was significant for follow-up periods beyond 12 weeks (SMD, 0.31; 95 % CI, 0.04, 0.59; 14 RCTs, I 2 = 69.0 %). Begg’s test was not statistically significant (p = 0.16) but Egger’s test showed evidence of publication bias (p = 0.04). The quality of evidence that mindfulness meditation is associated with a decrease in chronic pain compared with control is low overall and for both short- and long-term follow-up due to inconsistency, heterogeneity, and possible publication bias. A detailed table displays the quality of evidence for findings for each major outcome in Electronic Supplementary Material 2.
In order to present clinically meaningful results, we calculated the percent change in pain symptoms from baseline to follow-up for mindfulness meditation and comparison groups for each study and displayed findings in Table 2. We then calculated the overall weighted mean percent change for mindfulness meditation groups versus comparison groups for effects of meditation for pain at longest follow-up. The mean percent change in pain for meditation groups was −0.19 % (SD, 0.91; min, −0.48; max, 0.10) while the mean percent change in pain for control groups was −0.08 % (SD, 0.74; min, −0.35; max, 0.11). The p value for the difference between groups was significant (p = 0.0031).
Depression
Depression outcomes were reported in 12 RCTs [29, 31, 33, 34, 45, 46, 48, 49, 51–53, 56]. Overall, meditation significantly lowered depression scores as compared with treatment as usual, support, education, stress management, and waitlist control groups (SMD, 0.15; 95 % CI, 0.03, 0.26; 12 RCTs; I 2 = 0 %). No heterogeneity was detected. The quality of evidence was rated as high due to lack of heterogeneity, consistent study results, and precision of effect (small confidence intervals).
Quality of Life
Sixteen studies reported mental health-related quality of life; the effect of mindfulness meditation was significant in the pooled analysis as compared with treatment as usual, support groups, education, stress management, and waitlist controls (SMD, 0.49; 95 % CI, 0.22, 0.76; I 2, 74.9 %). [32–34, 45–49, 52, 54, 56, 59, 60, 62–64]. Sixteen studies measured physical health-related quality of life [32–34, 36, 45–49, 52, 54, 56, 60, 62–64]. Pooled analyses showed a significant effect of mindfulness meditation as compared with treatment as usual, support groups, education, stress management, and waitlist controls (SMD, 0.34; 95 % CI, 0.03, 0.65; I 2, 79.2 %). Both quality-of-life analyses detected substantial heterogeneity, and the quality of evidence was rated as moderate for mental health (small confidence intervals, more consistent results) and low for physical health-related quality of life.
Functional Impairment (Disability Measures)
Four studies reported poolable disability scores from the Roland-Morris Disability Questionnaire and the Sheehan Disability Scale [33, 36, 47, 55]. The difference between the mindfulness and comparison groups in follow-up was not statistically significant (SMD, 0.30; 95 % CI, −0.02, 0.62; I 2 = 1.7 %), although the results approached significance. No heterogeneity was detected. The quality of evidence was rated low due to imprecision and small total sample size.
Analgesic Use
Only four studies reported use of analgesics as an outcome. In a study of MBSR for treatment of chronic pain due to failed back surgery syndrome [55], at 12-week follow-up, the analgesic medication logs of the intervention group documented a decrease in analgesic use compared with those in the control group (−1.5 (SD = 1.8) vs. 0.4 (SD = 1.1), p = <0.001). A study of mindfulness meditation and cognitive-behavioral therapy vs. usual care for low back pain [35] reported that the mean morphine equivalent dose (mg/day) of opioids was not significantly different between groups at both 8 and 26 weeks. Likewise, a trial of MBSR for back pain [38] found no significant difference between groups in self-reported use of pain medication. Finally, a trial of mindfulness-oriented recovery enhancement (MORE) for chronic pain of various etiologies [44] found intervention participants significantly more likely to no longer meet criteria for opioid use disorder immediately following treatment (p = 0.05); however, these effects were not sustained at 3-month follow-up.
Adverse Events
Only 7 of the 38 included RCTs reported on adverse events. Four stated no adverse events occurred [36, 47, 50, 57]; one described that two participants experienced temporary strong feelings of anger toward their pain condition and two of the participants experienced greater anxiety [46]; two studies recorded mild side effects from yoga and progressive muscle relaxation [35, 38].
Study Characteristic Moderators
Meta-regressions were run to determine if changes in pain outcomes systematically differed by several subcategories. There was no difference in effect on pain between MBSR (16 studies) and MBCT (4 studies; p = 0.68) or other types of mindfulness interventions (10 studies; p = 0.68). When comparing MBSR (16 studies) to all other interventions (14 studies), there was also no difference in effect (p = 0.45). As stated in more detail above, medical conditions reported included fibromyalgia, back pain, arthritis, headache, and irritable bowel syndrome (IBS). Meta-regressions did not suggest differences between headache (six studies) and other conditions (p = 0.93), back pain (eight studies) and other conditions (p = 0.15), and fibromyalgia (eight studies) and other conditions (p = 0.29). Gender composition (% male) had no association with effect on pain (p = 0.26). The total length of the intervention program ranged from 3 to 12 weeks (mean was 8 weeks). Meta-regression did not suggest differences between high-frequency interventions and medium- (p = 0.16) or low-frequency (p = 0.44) interventions. No systematic difference in effect on pain between adjunctive therapy and monotherapy (p = 0.62) or between adjunctive therapy and interventions where this was unclear (p = 0.10) was found. Finally, there was no systematic difference in effect whether the comparator was treatment as usual, waitlist, or another intervention (p = 0.21).

Dr. Alex Jimenez's Insight
Chronic stress is a massive issue in the United States and it has had a detrimental impact on the overall health and wellness of the American population. Stress can affect different areas of the body. Stress can increase heart rate and cause rapid breathing, or hyperventilation, as well as muscle tension. Additionally, stress triggers the "fight or flight" response, which causes the sympathetic nervous system to release a mixture of hormones and chemicals into the body. Fortunately, chiropractic care can help with stress management. Chiropractic treatment activates the parasympathetic system which calms the "fight or flight" response. Furthermore, chiropractic care can help reduce muscle tension, improving chronic pain symptoms.
Discussion
In sum, mindfulness meditation was associated with a small effect of improved pain symptoms compared with treatment as usual, passive controls, and education/support groups in a meta-analysis of 30 randomized controlled trials. However, there was evidence of substantial heterogeneity among studies and possible publication bias resulting in a low quality of evidence. The efficacy of mindfulness meditation on pain did not differ systematically by type of intervention, medical condition, or by length or frequency of intervention. Mindfulness meditation was associated with statistically significant improvement in depression, physical health-related quality of life, and mental health-related quality of life. Quality of evidence was high for depression, moderate for mental health-related quality of life, and low for physical health-related quality of life. Only four studies reported on change in analgesic use; results were mixed. Adverse events in the included RCTs were rare and not serious, but the vast majority of studies did not collect adverse events data.
This review has several methodological strengths: an a priori research design, duplicate study selection and data abstraction of study information, a comprehensive search of electronic databases, risk of bias assessments, and comprehensive quality of evidence assessments used to formulate review conclusions. One limitation is that we did not contact individual study authors; results reported in the review are based on published data. We excluded conference abstracts which do not contain enough data to evaluate study quality. In addition, we included only studies published in English.
The included studies had many limitations. Thirteen of the thirty-eight studies were rated as poor quality, primarily due to lack of ITT, poor follow-up, or poor reporting of methods for randomization and concealment of allocation. The authors of ten studies reported inadequate statistical power to detect differences in pain outcomes between mindfulness meditation and the comparator; the authors considered these pilot studies. Ten other studies did not report a power calculation. Sample sizes were small; 15 studies randomized fewer than 50 participants.
More well-designed, rigorous, and large RCTs are needed in order to develop an evidence base that can more decisively provide estimates of its effectiveness. Studies should enroll samples large enough to detect statistical differences in outcomes and should follow-up with participants for 6 to 12 months in order to assess the long-term effects of meditation. Adherence to mindfulness practice and simultaneous use of other therapies should be monitored frequently. Intervention characteristics, including the optimal dose, have also not yet conclusively been established. In order to detect intervention specific effects, studies need to have attention-matched controls. Smaller trials may be conducted to answer these questions. Other outcomes that were outside the scope of this review may be important to explore. As the impact of mindfulness may be related to the appraisal of the pain, it may be useful for future trials to focus primary outcomes on symptoms associated with pain such as quality of life, pain-related interference, pain tolerance, analgesic, and related issues such as opioid craving. Future publications on RCTs of mindfulness meditation should adhere to Consolidated Standards of Reporting Trials (CONSORT) standards.
Only three RCTs attributed minor adverse events to mindfulness meditation. However, only 7 of the 38 included RCTs mentioned whether adverse events were monitored and collected. Thus quality of evidence for adverse events reported in RCTs is inadequate for a comprehensive assessment. Given published reports of adverse events during meditation, including psychosis [67], future trials should actively collect adverse events data. In addition, a systematic review of observational studies and case reports would shed additional light on adverse events during mindfulness meditation.
Further research examining the effect of mindfulness meditation on chronic pain should also focus on better understanding whether there is a minimum frequency or duration of meditation practice for it to be effective. While recent studies have yielded similar positive effects of mindfulness for pain, these effects tend to be small to medium and based on a body of evidence that is, at best, of moderate quality. A potential way to advance research on chronic pain would be to improve intervention and control group descriptions, identify different effects of various components of complex interventions, and work toward a standard criterion for assessing therapeutic gain [68]. Head-to-head trials that compare mindfulness interventions of a similar category but with variations in components or dose may be helpful to tease out the most effective elements of these interventions [69].
Similar to previous reviews in this area, we conclude that while mindfulness meditation interventions showed significant improvements for chronic pain, depression, and quality of life, the weaknesses in the body of evidence prevent strong conclusions. The available evidence did not yield consistent effects for pain outcomes, and few studies were available for forms of mindfulness meditation other than MBSR. Quality of evidence for the efficacy of mindfulness interventions in reducing chronic pain is low. There was higher quality evidence of the efficacy of mindfulness meditation on depression and mental health-related quality-of-life outcomes. This review is consistent with previous reviews concluding that more well-designed, rigorous, and large RCTs are needed in order to develop an evidence base that can more decisively provide estimates of the efficacy of mindfulness meditation for chronic pain. In the meantime, chronic pain continues to pose a tremendous burden on society and individuals. A novel therapeutic approach for chronic pain management such as mindfulness meditation would likely be welcomed by patients suffering from pain.
Electronic Supplementary Material
Ncbi.nlm.nih.gov/pmc/articles/PMC5368208/
Compliance with Ethical Standards
Funding and Disclaimer
The systematic review was sponsored by the Department of Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury (contract number 14-539.2). The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the views of the Department of Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury.
Authors Statement of Conflict of Interest and Adherence to Ethical Standards Authors
Authors Hilton, Hempel, Ewing, Apaydin, Xenakis, Newberry, Colaiaco, Maher, Shanman, Sorbero, and Maglione declare that they have no conflict of interest. All procedures, including the informed consent process, were conducted in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000.In conclusion, stress can ultimately affect our overall health and wellness if not managed properly. Fortunately, several stress management techniques, including chiropractic care and mindfulness meditation, can help reduce stress as well as improve chronic pain associated with stress. Chiropractic treatment is an important stress management technique because it can calm the "fight or flight" response associated with chronic stress. The article above also demonstrated how mindfulness meditation can be a fundamental stress management technique for improving overall health and wellness. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez

Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.

