




When the northern hemisphere winter approaches, millions head for the slopes. With that in mind, El Paso, TX. Chiropractor, Dr. Alexander Jimenez looks at what recent research has to say regarding injury and injury prevention...
But with increasing snow sport participation comes an elevated rate of traumatic injury as well as the information points to a substantial risk. Figures from US ski hotels revealed that in 2002, an estimated 77,300 ski and 62,000 ski injuries were treated in US emergency departments alone, such as 10,700 traumatic brain injuries(3). Still another study found that snowboarding is responsible for an estimated 25% of non-fatal outdoor injuries requiring emergency care(4).
Studies conducted in a number of countries across Europe and North America have suggested that the risk of injury for skiers and snowboarders is approximately 2 to 4 injuries per 1000 participant times, with the maximum threat in snowboarders(5-9). Children and teens at the 7-17 years age bracket appear to have higher rates of injury than younger and older participants(2).
There is recent evidence that the incidence of traumatic brain injury and spinal cord injury in skiing and snowboarding is increasing worldwide. This growth in severe injuries may be associated with greater risk-taking, such as jumping and acrobatic activities, both on new terrain and in snow resorts/parks specifically made for snowboarding(15).
Typical Injuries Sustained In Snow Sports
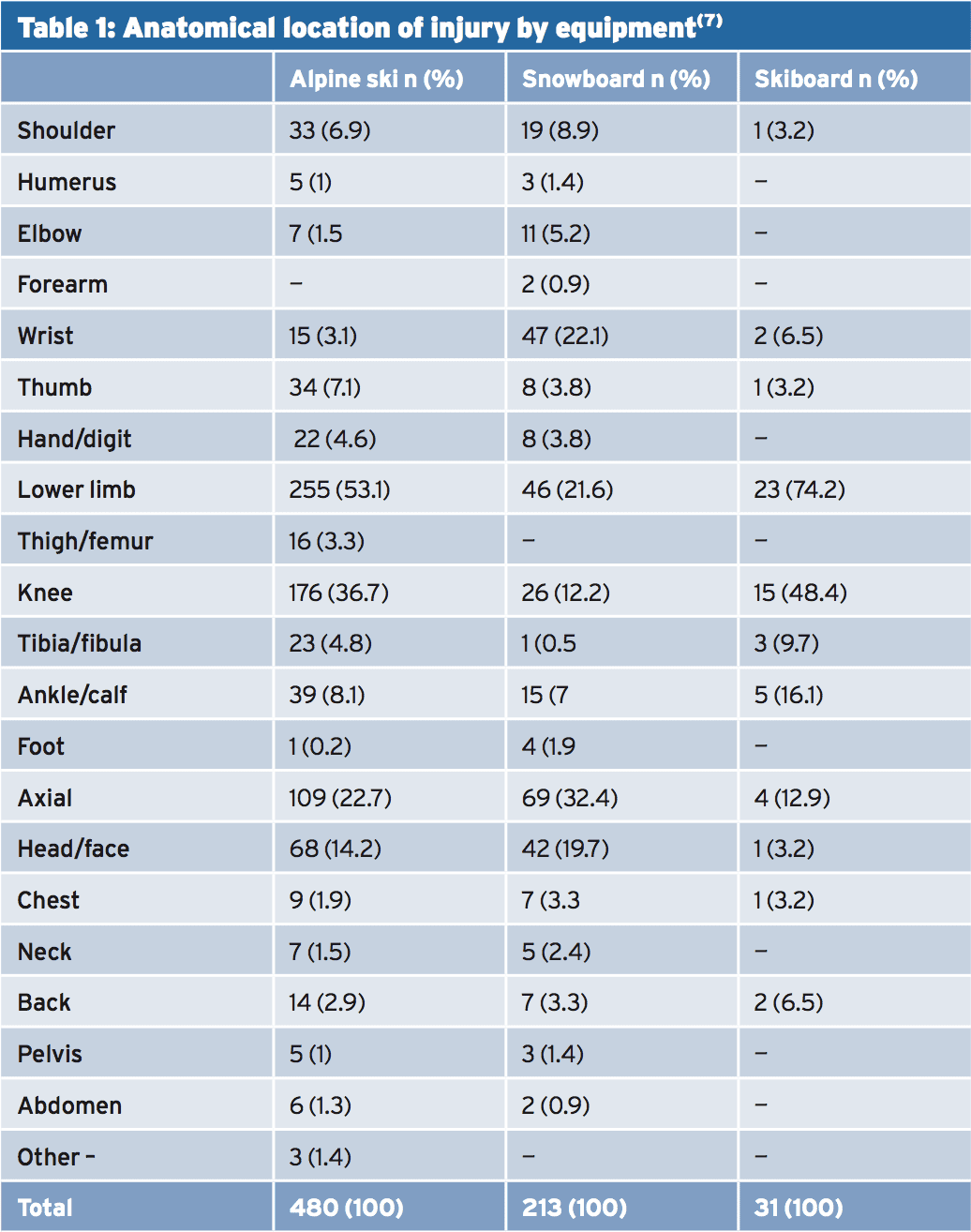
A number of reviews have been published that summarize the epidemiology of skiing and snowboarding injuries. Skiers tend to maintain injuries to the lower extremities; snowboarders, on the other hand, are much more likely to sustain injury to the upper extremities (see Figure 1)(16-17). Knee injuries are the most frequent type of injury in ski and constitute around 36% of all ski injuries, according to the literature(18). Snowboarders sustain more ripped ligaments and sprains/strains, brought on by a) position sideways on the board and b) that the absence of a safety binding that opens on its own in the event of a collapse. In a snowboard autumn, the wrists are particularly vulnerable to trauma, especially on impact.
Personal details, snow sports-related factors, diagnosis, and treatment have been recorded, and control data were gathered at random from uninjured people at all three areas. A total of 732 accidents were listed at 674 people and the injury rate for the study was 3.7 injuries per 1000 skier days -- very much in accordance with the studies above(5,6,8). Yet again, snowboarders lasted more injuries to the upper limb and axial areas than their skiing counterparts, also ski- boarders and snowboarders also suffered a higher incidence of fracture. Table 1 demonstrates how these injuries were broken down by sport type and anatomical location.
Injury Trends Over Time
The injury rates were assessed as mean days between injuries (MDBI -- the lower the number, the greater the injury rate). The findings were as follows:
● The average MDBI for all harms among snowboarders has been 345 as compared with 400 for skiers. The most frequent type of harm for snowboarders was a wrist injury (MDBI, 1258), although for skiers it had been an anterior cruciate ligament (ACL) sprain (MDBI, 2332).
● Wrist injuries accounted for 27.6% of all snowboard injuries and 2.8 percent of skiing injuries.
● ACL injuries composed 1.7% of all snowboard injuries and 17.2% of skiing injuries.
● Among snowboarders, more wrist injuries, shoulder soft tissue injuries, ankle injuries, concussions, and clavicle fractures were seen, while skiers had more ACL sprains, medial collateral ligament (MCL) sprains of the knee, lateral collateral ligament (LCL) sprains of the knee, lower extremity contusions, and tibia fractures.
● There was a trend towards an increased incidence of clavicle fractures and a decrease in MCL injuries and ankle injuries among snowboarders over time.
● Skiers had a decrease in thumb metacarpophalangeal-ulnar collateral ligament (MCP-UCL) injuries and MCL injuries of the knee over time.
● The highest rate of injury was among young, inexperienced, female snowboarders.
Overall, whilst injury rates in snowboarders have fluctuated over time, they now remain higher compared to skiers. This may be partly because of changing demographics -- snowboarding is frequently portrayed as a youthful, 'trendy' sport and the data indicates that injured snowboarders were significantly younger, less experienced, and more likely to be female than wounded skiers or snowboard management participants. The growth in rates of clavicle fracture might be connected to a heightened interest in snowboarding acrobatic/airborne maneuvers.
Injury Prevention In Snow Sports
Snowboarding equipment -- Since its inception, snowboarding has always been associated with a higher incidence of upper limb injuries compared to alpine skiing, with the wrist being the single commonest site of injury. In case of a collapse, the natural tendency for a snowboarder is to stretch out (and land on) the hand. Back in 1999, the evidence indicated that less than 10% of snowboarders were utilizing wrist guards to defend the wrist in these falls, despite there being a few epidemiological and laboratory evidence to support their use(22-24). With an increasing emphasis on security, you may think that the situation now is radically different but the evidence is less encouraging.A 2011 meta-study by US researchers studied all of the published literature about wrist guard use, trauma prevention, the biomechanical effects of wrist guards, and the various kinds of wrist guards commercially accessible for snow- boarders(25). The authors concluded that the use of protective equipment for the wrist is a helpful method for preventing injury. However, they pointed out that while numerous studies looked at the impact of wrist guards, there was no consensus about which particular kind of wrist guard would be most effective; the vast majority of the studies did not mention a brand name or a description of the type of wrist protector that was used by participants. It was also apparent that the literature generally reported low usage of wrist guards by snowboarders -- as low as 6 percent -- possibly because of aesthetics, societal acceptance, match or wrist guard and availability.
Some research has suggested that using wrist guards might increase the possibility of sustaining an elbow, upper arm or shoulder injury -- by transferring the loading during a fall further up the arm. On the other hand, the evidence for this can be conflicting and has not yet been confirmed in a controlled trial or well-designed prospective study and the present best guidance for snowboarders is to use a wrist guard to help avoid injury.
Skiing equipment -- Injury prevalence among skiers has declined over a few decades, largely because of improvements in ski gear, particularly boots and bindings; proof proves that modern bindings decrease the incidence of foot, ankle and lower tibial injuries providing they are properly mounted, adjusted and maintained(26,27). Many accidents are the result of poorly adjusted bindings; in one analysis of adult lower extremity equipment- related injuries it had been determined that in 96% of cases the ski bindings did not release when the accident happened(28). Non-release of bindings has also been reported as an injury contributor in different studies of the two youths and adults. In one study, skiers younger than 13 decades of age with poorly adjusted bindings were much more likely to be injured than children with correctly adjusted bindings(29). Unsurprisingly, therefore, some investigators have proposed that a professional should adjust children's and beginners' ski bindings at the start of every lesson and that these groups should be taught to check their bindings at the beginning of each ski day(30).
Snowboarding and skiing equipment -- One place where there's little doubt over powerful equipment-based harm prevention is helmet use. A new systematic review found that helmets significantly lessen the risk of head injury(31). Skiers and snowboarders wearing a helmet were far not as likely to have a brain injury, and this threat was further reduced when research which included children younger than 13 decades of age were included. Overall, the pooled results showed that helmet use reduces the chance of head injury by around 35%.
Some researchers have raised concerns that while helmet use during skiing and snowboarding reduces head injury rates, it may increase the risk of cervical spine injuries. However, these concerns are not supported by many of case control studies(32-35) and also a 2010 systematic review also concluded that helmets weren't related to an increased risk of neck injury(31). Moreover, there's also no proof that helmet usage in skiing and snowboarding is connected with riskier behaviour (36,37). The obvious conclusion here is that helmet usage ought to be considered compulsory at all times where safety is an issue.
Physical Conditioning: Snow Sports & Injury Prevention
Power, endurance and cardiovascular fitness are all central components in sports injury prevention throughout a vast range of sports, and yet in snow sports, there appears to be a much greater emphasis on equipment-based and third party alternatives. A comprehensive and systematic overview of the literature printed in 2013 looked at injury prevention recommendations specific to recreational Alpine skiers and snowboarders. The attention was to discern recommendations that concentrated physical fitness, exercise and/or training in preventing musculoskeletal injuries in these two sports(38). Studies were included if they dealt with injury prevention, recreational Alpine skiing or snow- boarding and musculoskeletal injuries and articles on elite athletes were excluded.Overall, 80 recommendations for the prevention of musculoskeletal injuries in recreational Alpine skiers and snowboarders were identified and classified into five main categories:
● Equipment use(n=24)
● Education and knowledge(n=11)
● Awareness and behavior
● Experience(n=10)
● Third-party involvement(n=20)
● Education and knowledge(n=11)
● Awareness and behavior
● Experience(n=10)
● Third-party involvement(n=20)
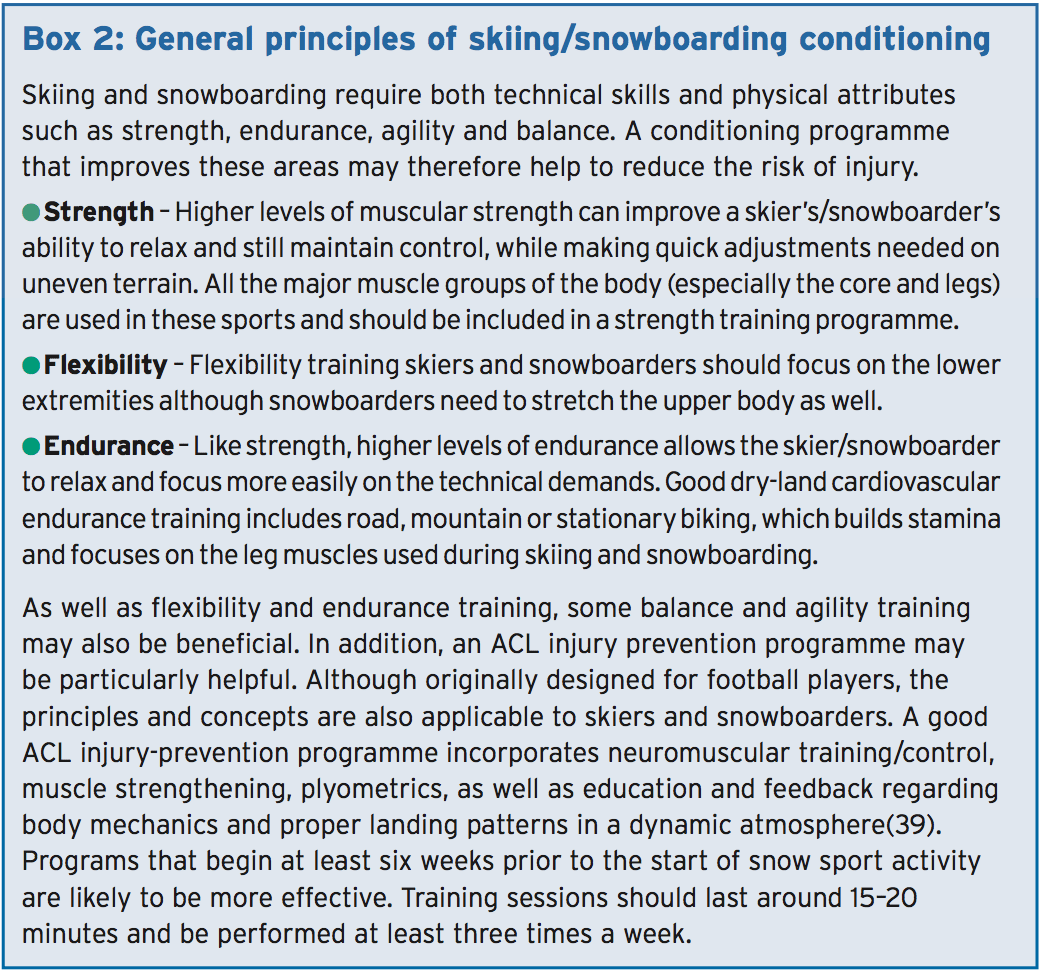
Amazingly, there was no research that made recommendations pertaining to physical fitness, exercise and/or training per se, or its role in preventing injury! The authors commented thus about the frequent recommendations for preventing ski and snowboarding injuries by an equipment-based or third party approach: "The dominance of equipment-related steps in the injury prevention literature may be rationalized from a sports biomechanics perspective, because these activities involve high velocities and impact forces. Nonetheless, this also suggests a need for proper levels of power, conditioning and endurance to fulfill the technical requirements of the sports." To put it differently, while it makes sense to take precautionary measures regarding proper equipment use, consciousness, behavior etc, neglecting essential physical conditioning could be counterproductive. Unfortunately, there are no peer-reviewed studies about which type of conditioning system is the most suitable for snow sport injury prevention, but some of the general principles that are very likely to be useful are summarized in Box 2 below.
Overview
Skiing and snowboarding by their very nature carry a substantial risk of injury, which could sometimes be serious. The most common injuries are to the knees in skiers and wrists in snowboarders, and the rate of injury is greatest in novices, the less experienced and the young. Along with equipment-based measures, (eg bindings when skiing and wrist guards when snowboarding) is critical for reducing injury risk. Helmet use is also vital to reduce the incidence and severity of head injury in both skiers and snowboarders. In addition a proper pre-skiing/snowboarding conditioning system may also play an important part in ensuring a visit to the slopes is memorable for all the right reasons.References
1. National Ski Areas Association. Kottke National End of Season Survey 2010/11: Final Report. Table 6: Estimated US Ski Injury Skier Visits by Region 1978/79 – 2010/11. http://www.nsaa.org/nsaa/press/historical-visits.pdf
2. Inj Prev 1996;2(4):286-9
3. J Trauma 2005;58(1):112-8
4. Wilderness Environ Med 2008;19(2):91-8
5. Br J Sports Med 2004;38(3):264-8
6. Sports Med 2004;34(2):133-9
7. Br J Sports Med 2002;36(2):135-40
8. Am J Sports Med 2004;32(1):96-103
9. Am J Sports Med 1995;23(5):597-600
10. Am J Surg 2009;197(5):560-4.
11. Inj Control Saf Promot 2004;11(4):281-5
12. Injury 2003;34(12):892-6
13. National Ski Areas Association. Facts About Skiing/Snowboarding Safety: Updated March 2006. http://www.nsaa.org/nsaa/press/0506/facts-about-skiing-andsnowboarding.asp
14. Sports Health. 2009 Nov;1(6):486-92
15. Inj Prev 2007(6);13:368-75
16. Acta Orthop Scand 2001; 72: 657–660
17. Am J Sports Med 1999; 27: 94–97
18. Am J Sports Med 1999; 27:381–389
19. Schweiz Monatsschr Zahnmed. 2013;123 (7-8):655-9
20. Paediatr Child Health 2012;17(1):35-6
21. Am J Sports Med. 2012 Apr;40(4):770-6
22. Skiing trauma and safety. 12th volume. Philadelphia: American Society for Testing and Materials, 1999:141–9
23. Am J Sports Med 1998;26:825–30.
24. J Trauma 2000;48:1109–14
25. Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):149-57
26. Sports Med 1999;28(1):35-48.
27. Aust Fam Physician 2003;32(7):499-502.
28. J Orthop Sci 2002;7(1):1-5
29. Am J Sports Med 1999;27(5): 644-50.
30. Sports and Recreation Injury Prevention Strategies: Systematic Review and Best Practices; Executive Summary. Vancouver: BC Injury Research and Prevention Unit, 2001.
31. CMAJ 2010;182(4):333-40
32. BMJ 2005;330(7486):281
33. Semin Neurol 2000;20(2):233-45
34. Epidemiology 2008;19(2):270-6
35. JAMA 2006;295(8):919-24
36. Accid Anal Prev 2005;37(1):103-8.
37. Inj Prev 2007;13(3):173-7
38. Sports Med. 2013 May;43(5):355-66
39. Br J Sports Med. 2008 Jun; 42(6):394-412
