




Science chiropractor, Dr. Alexander Jimenez has a look at a patient with pain in her calf -- and brand-new jogging shoes.
A 33-year-old female presented to the clinic with a tight and painful medial aspect of the left calf. The patient complained that she believed she had been suffering from 'shin splints'. The pain had begun after an especially challenging course run over rocky and hilly terrain. No pain was noticed during the running session nevertheless, the pain began the following day. There was no pain in the arch or ankle of the foot.
On clinical examination, the pain has been concentrated on the muscle belly of the flexor hallucis longus (FHL) muscle because it divides out from underneath the soleus. The pain was exacerbated by shoving off through walking and was evident on stretching ankle dorsiflexion with associated big toe dorsiflexion. Contraction of the large toe into plantar flexion although the ankle was also plantar bending also caused pain. She had been diagnosed with a strain of this FHL muscle. She had been back to complete running in 3 weeks.
What was intriguing to notice in this individual was that she had recently purchased new running shoes. The shoes she had bought (Asics Gel Kayano) would be the same ones she generally conducted with. However, she remarked that those she had bought were a half size bigger than the previous pair. When I asked her why she had purchased a larger pair of shoes, she clarified that the sales rep at the shoe shop had measured her foot length and noticed that the ideal foot was a half size larger than the left, and argued that she had a pair of shoes to match the larger foot to protect against any forefoot compression in the shoe.
What was important to me was the fact that the larger shoe on the left had actually resulted in the FHL muscle strain. The reason, I concluded, was that when operating on tight irregular surfaces, her left foot would have been sliding in the shoe more than the right foot as a result of excess length in the left shoe. This always would have led to her overusing the FHL to 'claw' her big toe into the sole of the shoe to reduce the shear and slipping of her foot. This could have overloaded the FHL sufficiently to cause a muscle strain.
The FHL Muscle
It's a flat bipennate muscle which courses obliquely under the soleus to appear over the medial side of the tibia. It's located in the deep posterior compartment of the lower leg with all the tibialis posterior and the flexor digitorum longus (FDL). All three tendons of the muscles emerge on the medial ankle to form what is known as ‘Tom, Dick and Harry’ (Tib Post, FDL and FHL). The tendons course through the tarsal tunnel on the medial side of the ankle and the FHL continues under the arch of the foot to insert onto the underside of the big toe.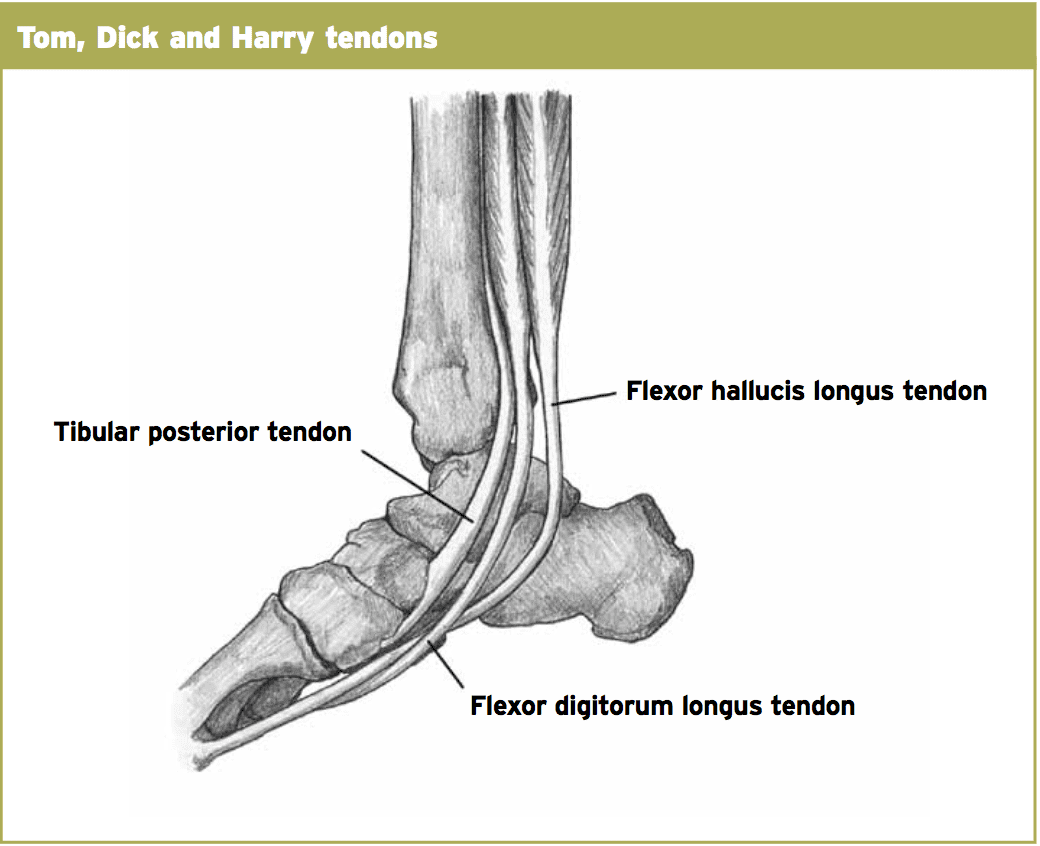
Cadaveric studies also show that in some people an attachment slip of the FHL muscle moves inferiorly to the anterior ankle (this has sometimes been known as the 'beef of their heel'). This accessory slide of muscle can also be irritated and impinged in the back of the ankle.
FHL Injuries
Stenosing tenosynovitis of the FHL is very common in ballet dancers on account of the replicate plantar flexion position that ballet dancers get into. This causes the tendon to constantly friction and interrogate against the bony structures of the talus and calcaneus. The identical difficulty has also been reported in athletes who spend a good deal of time in plantar flexion for example leaping athletes, equestrian athletes and space runners between numerous mountain runs.The tendon of the FHL can also develop nodules and little intrasubstance tears. What compounds these problems from the thoracic as it courses around the back of the ankle is the existence of a bony os trigonum that functions as a possible source of impingement into the FHL tendon.
Of further interest is that the uncommon muscle-tendon arrangement of the FHL that can project deep to the anterior ankle. The musculotendinous junction may become thickened and entrapped in the fibro-osseous tunnel -- the cork from the bottle syndrome.
Finally, injuries to the FHL musculo-tendinous junction and FHL limb has regularly been reported on MRI in post-ankle sprains. The mechanism of injury for this makes sense when one believes that the usual plantar flexion/inversion mechanism of ankle sprain will impinge the tendon in the posteromedial ankle and possibly harm the tendon and sheath construction.
Diagnosis
Often the pain at a FHL tendon begins insidiously and is found in the postero- medial ankle and it might radiate distally to the lateral arch (often being confused for plantar fasciitis).Often these patients are not going to have the early morning pain and stiffness evident with plantar fasciitis, so these may be utilized as a diagnostic tool in identifying FHL tendon injuries versus plantar fasciitis.
Swelling may be present in the medial ankle and the presence of a positive Tinels sign (tapping the posterior tibial nerve which reproduces foot tingling) are also evident.
The imaging methods of choice at FHL injuries is MRI to visualise both muscle and tendon injuries and tenography for tendon issues like stenosing tenosynovitis and stomach tears. En pointe lateral foot x-rays are required in dancers to exclude anterior impingement syndromes. Dynamic ultrasound of the FHL tendon may also demonstrate a stenosis of the thoracic or a low-lying attachment slide of the FHL muscle.
Treatment
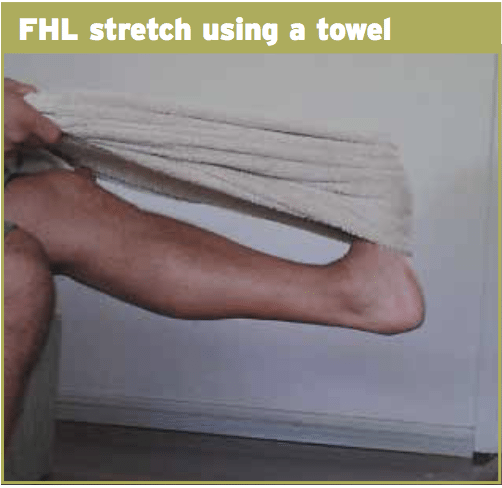
Normally the conservative management of FHL tendon problems originally involves modified action, NSAIDS, protective arch strapping with hallux dorsiflexion check straps, trigger point releases of their FHL muscle, direct strengthening of their FHL correction and muscle of any subtalar or talocrural joint dysfunctions.To stretch the FHL, the foot is placed up against a rolled towel or step so that the ball of the foot is on the floor however the big toe is forced to dorsiflexion. Then bend the knee and knee to spend the ankle into dorsiflexion. Push the foot against the towel resistance into ankle plantar flexion and big toe plantar flexion.

Conclusion
FHL tendon injuries are a common injury in professional dancers, less common in athletes and almost non-existent in non-athletes. It can be impinged by continuous plantar flexion positions particularly if the ankle has a sizable or medially displaced os trigonum or when the muscle belly of the FHL jobs deep down into the posterior ankle. Impingements poor to the ankle and at the arch are much less common.The case study presented highlighted an unusual but intriguing mechanism of harm into the FHL muscle building. Wearing shoes which are too large will create a 'sliding' or ' 'shear' of the foot in the shoe. This may result in excess FHL action as the big toe 'grips' the shoe to prevent this excessive sliding and shear.
