




The narrative of Anna's dodgy shoulders holds two lessons: the value of superior stability and the value of a rigorous strategy by sports therapists. Core chiropractor, Dr. Alexander Jimenez takes a closer look.
Anna, a tall, slender 15 year old, came for her appointment to see me with her mom. Together they explained that she had a national swim meet in two weeks, but that her shoulders were really giving her problems and had been doing so for about three months. Throughout this time Anna had improved her training before the state championships, where she had done surprisingly well in different freestyle and medley events, considering how little training she'd done before.
Anna seemed quite gangly, with stooping posture, a gait that looked very sloppy (knees bending backwards & unstable pelvis) with rather large feet... it was like she was designed for the pool!
She complained that her shoulders clicked, and sometimes felt like they 'popped out of joint' when she was doing a difficult sprint session. They tended to hurt largely as an ache, often after she'd cooled off, but occasionally during her warm-up. They could feel very tight when she would wake up.
A GP they'd visited prescribed anti-inflammatory medication, told her she'd rotator cuff tendinitis inflammation), and delivered her for stretching and ultrasound therapy. Anna's trainer was keen to talk with me about what was going on with his star swimmer and whether she'd be ready for the nationals in two weeks' time.
Deciding What's Wrong
The moment a clinician was presented with the injury, their mind begins to play with different diagnostic scenarios. This process, known as 'clinical reasoning', constitutes the subjective (from interview) and objective (from hands on testing or other investigative processes) information from the customer, and gradually develops an evidence-based rationale for the most likely diagnosis. The identification forms the building block for most future management; therefore: no accurate diagnosis, no good result.In this instance, based on what we understood from Anna's story, we needed to assess the validity of the following potential diagnoses, in order of best likelihood (there are other possible shoulder pathologies, but I thought these were the very likely):
Multi-Directional Instability (MDI) Of The Gleno-Humeral Joint
This was the most powerful likelihood. How Anna has been having trouble in both shoulders indicated a probable genetic/familial component and MDI tends to occur on either side in shoulders where there is a genetic tendency towards hyper-mobility. Excessive translation (shearing movement) and also inferior centering of the head of humerus (the 'ball' in the shoulder socket) in all directions leads to gradual destruction of the cartilaginous rim (the labrum) and rotator cuff tendon. Pain and clicking effect, together with the head of humerus in impact repeatedly popping slightly in and out of the joint throughout the swimming stroke.Uni-Directional Instability Of Gleno-Humeral Joint
Excessively protracted posture (round shoulders destroy the uterus!) Can cause the middle of rotation of the head of humerus slowly to drift forwards. The subscapularis muscle loses its ability to control it, straining on the joint capsule and loosening, which soon leads to instability. Finally the head of humerus will start to pop out, or even the rotator cuff tendon would impinge (catch) below the acromion (top outer edge of the shoulder blade), resulting in pain and clicking. Uni-directional instability are more likely to occur in one overloaded shoulder, especially on the non-dominant arm at a bilateral sport, not in two.Superior Labrum Anterior Posterior (SLAP) Lesion
Looseness in the front part of the shoulder joint may also induce the long head of biceps tendon and the lower part of the joint capsule, which ends up destabilizing the link of the cartilage on the rim into the bony glenoid. However, this kind of shoulder injury more commonly afflicts throwing athletes and, again, generally presents on only one side.Rotator Cuff Impingement Or Tendinitis
According to Anna's account of her symptoms, this is likely to be a secondary issue caused by instability: uni- or multi- directional. In fact gleno-humeral instability is a much under-diagnosed source of rotator cuff impingement or tendinitis. Anna, at age 15, is quite unlikely to have tearing or significant degenerative change of her rotator cuff, even though it might be inflamed.Clinical Testing
Tests performed by an experienced physiotherapist will greatly help to decide or confirm their hypothesis. We utilized the following tests to help us work out which of the above diagnoses finest clarified Anna's issue.
Sulcus test (gently drawing the head of humerus out of the socket) determines the extent of MDI and loss of normal negative-suction joint pressure, and compares joint looseness on left and right sides of the body. We did other general hypermobility testing (eg, elbows and thumbs) to confirm Anna’s hypermobile status (which is shared by 10
per cent to 20 per cent of the population).
Apprehension testing: the test is positive if a backwards (posterior) glide of the head of humerus in a ‘stop’ sign takes away discomfort.
Posterior laxity testing: determines the extent of instability in the context of MDI. Long head of biceps: (moving the bent arm against resistance in various positions). Clicking and pain might reveal the compromised integrity of the bicep muscle attachment at the shoulder rim.
Cervical and thoracic spine: The therapist can feel for stiffness through the mid- to upper spine. Stiffness here is very common and disrupts the normal movement of the shoulder joint.
Cervical and thoracic spine: The therapist can feel for stiffness through the mid- to upper spine. Stiffness here is very common and disrupts the normal movement of the shoulder joint.
- rotator cuff flexibility
- impingement
- stability
Short-Term (Pre-Competition) Aims Of Management
Having completed the above tests we reasoned that Anna's main problem was indeed a multi-directional uncertainty of the shoulder joint, suspended in being genetically hypermobile. This had led to secondary annoyance and impingement of the rotator cuff tendon.After we were fairly certain of our diagnosis, we devised a management program, originally focused on the big upcoming competition; thereafter looking to supply a long-term resolution of Anna's injuries. Trying to be realistic about what we could achieve in just two weeks, we limited our pre-competition approach to three areas:
1. Establish Accurate Diagnosis As Early As Possible
This was essential. It may require another opinion from a sports doctor, and possibly scans: ultrasound for rotator cuff tendon ethics, CT arthrogram/ / MRI for labral (cartilage) tears, X-ray to view shallowness of the glenoid socket.2. Minimize Short-Term Pain & Additional Joint Breakdown
We used trigger-point massage and work on the rotator cuff to get rid of pain from active movements, impingement positions and finally, Anna's swimming stroke. We undertook deep-tissue massage of this key back, torso, torso, shoulder and arm muscles. We mobilized the mid- and upper back.We instantly stopped Anna from ongoing any dangerous or aggravating practices, such as bad sleeping positions (along with her shoulders at extreme positions and being leant on poorly); carrying too heavy a backpack; and any dangers from different sports she might be playing.
We assessed Anna's stretching regime, believing it was likely that most of her moves would be damaging because of her bad control. As a better alternative we taught her to do self- trigger point therapy and massage.
We taped the shoulder blades for support out of the pool and to assist Anna in re-educating her posture. In the pool we experimented with a different kind of tape for joint support and to help her get feedback on joint position.
We discussed with Anna's coach a short-term decrease in her training load and intensity for pain control, and established a focus on quality not quantity during the run-up to the competition (for instance, minimizing her butterfly training due to the greater loads this stroke places on the joint structures at the front of the shoulder).
We used non-steroidal anti-inflammatories and ice after training as required.
3. Educate Anna, her parents and her coach
The key things to communicate were:- the nature of the shoulder problem, especially how normal and unstable shoulders differ structurally;
- the importance of posture;
- an overall appreciation of the strengths and weaknesses of her body-type: her flexibility, which is such a natural plus in her swimming, needed to be balanced by stability and strength. Muscle control and strength must become her focus or she would never establish herself as a competitive swimmer. She needed a paradigm shift from concentrating mainly on flexibility to focusing instead on technique, co- ordination, warm-up drills and home-based self-massage and triggering to deal with tightness.
Long-Term (Post-Competition) Aims Of Direction
We are confident that a full resolution of Anna's shoulder problem is possible, with a return to symptom-free swimming, and a complete training and competitive load. She'll likely need, a preventative regime to ensure she remains injury-free. Much like many athletes that have experienced sports accidents, Anna will have to get accustomed to taking responsibility for preventing a recurrence before the day she decides to hang up her goggles.We had three primary long-term tactical objectives.
1. Maximize the muscular control of her shoulder joint
This entails growing, together with Anna, her parents and her trainer, a graduated plan to combat weaknesses and lively instability.The retraining work should begin with local stability muscles, working around three key areas:
- Trunk (transversus abdominis)
- Scapula(lower trapezius and serratus anterior)
- Head of humerus (subscapularis)
This stability and strengthening work will take three to six months, divided into three phases:
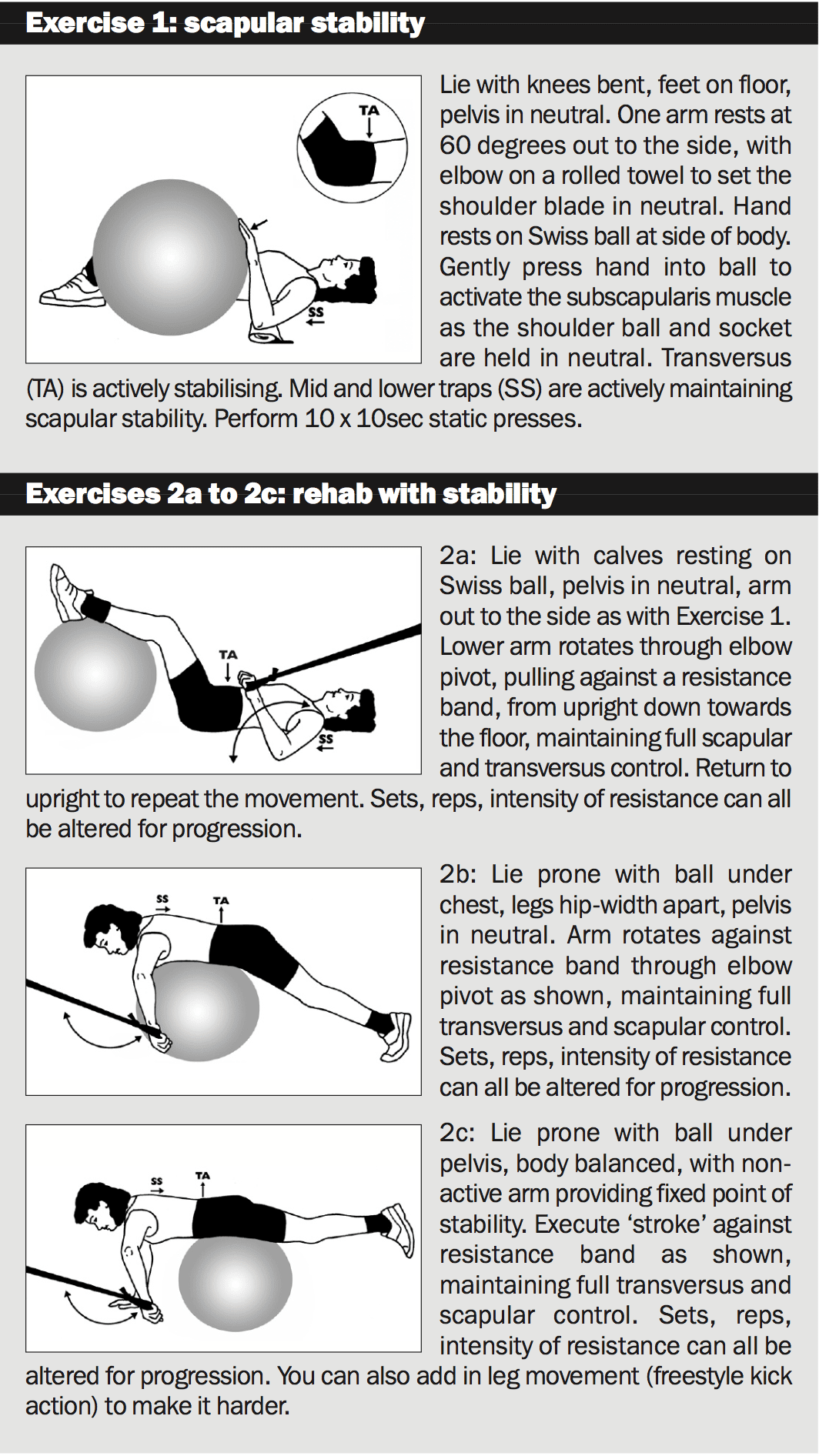
Activation - of proper muscles, as described previously. For example, if Anna didn't learn to activate the muscles controlling her shoulder blades, then she would perpetually tend towards downward turning, which makes it impossible for her subscapularis muscle to control the mind of humerus correctly. So the mid-lower traps (upward rotators of the shoulder blade) must be trained within the rhomboids for stability (see exercise 1 below).
Recruitment - of same stability muscles within rehab and dry-land swimming exercises. As local equilibrium improves, the exercises should slowly stress global strength and stability muscles. The quality of control remains a top priority as the exercises are progressed (see exercises 2a to 2c).
Regardless of whether the shoulders are symptomatic, Anna's off-season period will have to include a few weeks of stability and strength work from the lead-up to the start of swim training.
2. Resolve technique issues
Video analysis would be introduced through all 3 phases of rehabilitation training, in close liaison with the coach. It's critical that an athlete's knowledge and consciousness of good stability runs alongside their correction of poor technique, so they could understand and apply the muscle retraining to create necessary but often subtle modifications to movement mechanics. As an example, learning to hold the back and shoulders still while 'catching' the water through straight enhances scapular stability.3. Long-term flexibility management
Anna's priorities are her thoracic spine, back, chest and neck musculature, to enhance the stability of her trunk, shoulder blade and head of humerus. She would be likely to require maintenance physio and massage, particularly in periods of intense training and competition, in order to stay symptom-free.If Anna can conquer the hurdles in this phase of her career, she could open up for herself the chance to achieve what the shoulders of Ian Thorpe have: genetic hyper flexibility coupled with excellent control and strength, resulting in top level success.
The information contained in this publication is believed to be correct at the time of going to press. Whilst care has been taken to ensure that the information is accurate, the publisher can accept no responsibility for the consequences of actions based on the advice contained herein.
