




Exactly how effective are injury-prevention programs in soccer? El Paso, TX.s Scientific chiropractor Dr. Alexander Jimenez looks at the very latest evidence...
Football is the world's most popular team sport. Injuries are a significant issue for both amateur and professional players. Indeed, previous research has estimated that soccer players are among the most injury-prone athletes having an estimated injury rate of 17-24 accidents per 1000 playing hours(1). Nineteen per cent of all sports injuries which exist in the Netherlands are because of soccer(two) and in Britain alone, the expense of therapy and time lost from work owing to football injuries is estimated to be approximately #1billion annually(1)!
In a landmark study, researchers followed two Champions League teams and gathered data on 2,229 players over seven seasons to examine the injury profile of muscular injuries in soccer players(3). They also analyzed the gamers' training schedules and data out of their games to construct a detailed picture of the injury risks that were associated. The findings were as follows:
- 2,908 muscle injuries have been enrolled;
- Normally, a player sustained 0.6 muscle injuries each season (equating to around 15 muscle injuries per season at a squad of 25 players);
- Muscle injuries constituted 31 percent of all injuries and caused 27% of the total injury lack;
- Ninety-two per cent of muscle injuries affected the four Big muscle groups of the lower limbs: hamstrings (37 percent), adductors (23 percent), quadriceps (19%), and calf muscles (13%);
- Sixteen per cent of the muscular injuries were re-injuries; nonetheless, these re-injuries caused significantly longer absences than did the first injuries.
- The prevalence of muscular injury increased with age.
Given the high levels of trauma among football players (a risk that is increased during periods of match congestion) and the financial pressure of the modern game, it's perhaps unsurprising that medical team caring for players find that treatment of injuries in players is quite a frustrating and also a never-ending struggle. In addition, it clarifies why some players end up returning to contest prior to the injury has healed completely, setting the stage for injury recurrence, together with protracted absence of this participant from competition and training.
Injury Treatment
Treating injuries in football is both time- consuming and expensive, particularly at the elite level. And while there's a large literature on the epidemiology of sports injuries, established protocols for treating muscular injuries and assessment criteria for imaging, and a number of clinical and functional tests that could assist the health staff in deciding the optimal point where an athlete can be safely returned to full participation(5,6), the current guidelines haven't translated into a significant reduction in muscle injury levels in professional sports such as soccer.To simplify things further, the evidence indicates a new injury often occurs within a couple of weeks after return to contest, and typically costs the player more lost playing time than the key injury(7). The most probable reasons for this observation are likely associated with bodily alterations following the first injury, such as muscle stiffness and/or fatigue, scar tissue formation, biomechanical alterations, neuromuscular inhibition, as well as inadequate treatment -- for instance, overly aggressive or incomplete rehabilitation(8-10).
Injury-Prevention Programs
Even armed with knowledge that is up-to-date and the best technology is fraught with difficulty. Remembering the old adage that 'an ounce of prevention is worth a pound of cure', a alternative that is far better to attempt to prevent injuries from happening in the first place with an injury-prevention program. This is easier said than done. It is correct that there is an abundance of literature on the effectiveness of methods to avoid harm recurrence and muscle injury, such as enhancing flexibility eccentric and concentric exercises and drills. Despite this and apps like FIFA's 'The II' (see Box 1), the incidence of muscle injuries generally, and the recurrence rate particularly, remains stubbornly high(11-16).
From the analysis, 479 adult male amateur gamers aged 18-40 years have been split into two classes: the intervention group had been taught to do exercises focusing on core stability, bizarre training of thigh muscles, proprioceptive training, dynamic stabilization, and plyometrics with straight-leg orientation at every training session (2-3 sessions per week) through one season. The management team, meanwhile, continued their usual warm up.
As in the previous study, there were no significant differences in the percentage of players that are injured and injury rates between the two groups. What was intriguing was that in the intervention group, the price of injury treatment was 256 per participant. In the control group nonetheless treatment costs were twice at $606 per participant. The investigators commented that the cost savings in the intervention group may be the result of a rate of knee injuries, which have costs because of more lengthy rehabilitation periods and much more time lost at work compared to a number of different injuries.
Meanwhile, another study on an injury- prevention program (based on The II) in male amateur players had been printed in the end of last year(20). It discovered that (like the previous studies), an intervention program did not decrease the incidence of harm throughout the course of a season. However, such as the study, the players in the intervention group did incur less health care costs, although a justification for this finding wasn't given. As if to validate the confusion surrounding the value of injury-prevention programs for football players, then a recently published systematic overview of all of the previous studies released thus far fought to achieve a definitive conclusion(21). Six studies involving a total of 6,099 participants met the inclusion criteria and the results of these were conflicting two of the six studies (among large and one of moderate quality) reported a decrease in injury rates that were actual. Four of the six research an 'preventive effect', even though the effect of a single study wasn't statistically significant. Possible reasons for these contradictory findings might be subject choice (sex and level of ability), differences between the intervention programs implemented (content, training frequency and duration) and compliance with this application. What's clear, however, is that studies investigating the type and seriousness of exercises within an injury-prevention program are still required to reduce the incidence of accidents in soccer efficiently.
Good News On Prevention
Since the review study cited previously(21) was printed, two quite newly published studies on injury-prevention apps in soccer seem to provide more encouraging news -- for muscle injuries at least. In one, researchers studied elite players competing over two consecutive seasons, where the first (2008-2009) function as intervention period and the second, the management period (2009-2010)(22). In total, 26 (08/09) and 23 (09/10) elite male pro football players competing within the Scottish Premier League and European competition participated. The accident prevention training program was conducted twice weekly to the entirety of this season (58 avoidance sessions) and the results were compared with the control (no injury-prevention program) year.On first inspection, the results were disappointing, showing an increase in the complete number of accidents within the intervention period (88 vs 72). But this was largely because of the greater quantity of contusion injuries sustained inside the intervention season (44) compared with control season (23). Assessing like for muscular injuries that were significantly fewer were observed during the intervention season, which had been even more impressive given the larger squad size at the intervention season.
Another newly published study by Italian scientists who researched the effect of a two-tiered injury-prevention program on initial injury and re-injury prevalence in 36 elite male football players also causes encouraging reading(23). During the season prior to that examined in the study, there had been 27 muscle injuries in the group, which accounted for 58.7 percent of the total injuries: 13 of these had occurred throughout practice and 14 during matches. The general incidence of muscular injuries was 5.6 injuries/1000 hours of training/playing exposure and the effect was 106.4 times absence/1000 hours exposure.
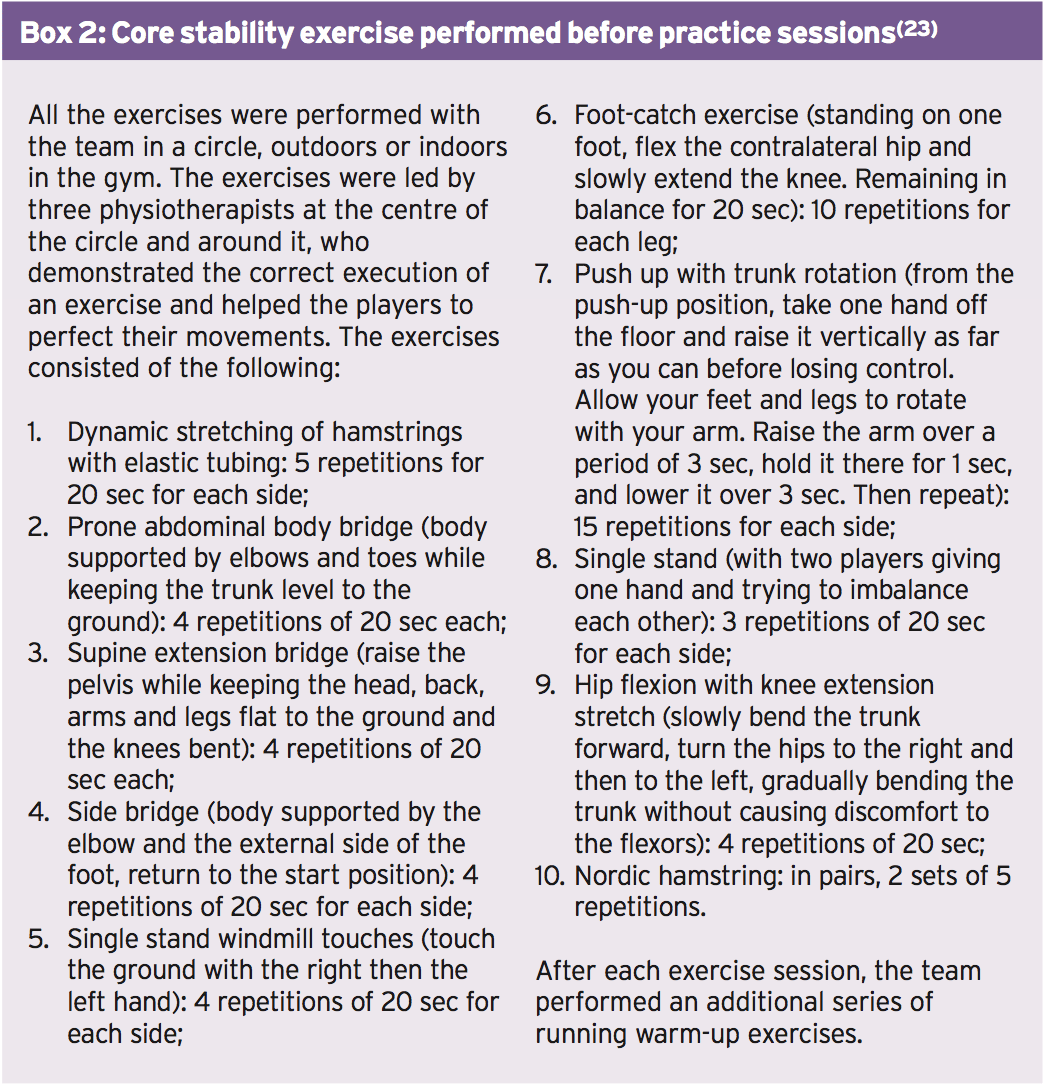
To try and decrease the speed of injury through the following season, the team doctor (also among the study's authors) found an injury-prevention program, conducted 2-3 times per week. This consisted of two elements: a collection of core stability exercises conducted by the whole group prior to each practice session (see Box 2) along with an individualized injury prevention program, which has been started after assessment with kinesiologic and diagnostic tests. At the start of the year, every athlete underwent testing of leg flexibility using the Ober evaluation, Thomas evaluation and straight-leg-raising [SLR] test(24-26). The prone instability test(27) was completed to show spinal instability along with the stork test (28,29) to assess sacroiliac dysfunction. Quadriceps and hamstring strength were measured isokinetically and attention was directed in evaluation of immunity of gluteus medius' power.
Results
Throughout the intervention season, a total of 64 injuries occurred -- 36 (56 percent) during practice and 28 (44%) during matches. Of them, 20 were muscle injuries, accounting for 31.3 percent of the total injuries; 14 of which occurred during practice and 6 during games. In all, three re-injuries happened and (15 percent of overall muscle injuries) and there were not any premature re-injuries. In comparison with the preceding season with no intervention-program set up, there was a reduction in the number of times and muscle injuries . Specifically, whereas muscle injuries accounted for 31 percent of harms they accounted for 59% of all injuries. Significantly, the number of injuries per 1000 hours of training and playing time was reduced by over half of 5.6 to 2.5. Meanwhile, the number of days fell by nearly two-thirds 106 into 37. The investigators put the success of this intervention down to three key aspects:- An injury prevention program that comprised of core stability exercises similar to those in 'The II' program but which differed in its two-tiered arrangement (group and individual sessions), allowing for intense and special training. In contrast, the combined results in research into The II app are probably because of the non- special content and ineffective intensity.
- The program's continuity of commitment by the players to both the group and individual areas.
- The addition of bizarre hamstring training in the group program (2 sets of 5 repetitions per week) combined with all the personalized application for players with a history of injury.
- Using ice baths in the conclusion of every training session
Summary & Recommendations
Injury treatment in aggressive soccer is equally costly and time-consuming also given the pressures of the game, injury avoidance is more important than ever. But, despite extensive published literature on harm prevention strategies and initiatives such as FIFA's 'The II', the injury rates in soccer remain high, especially in the higher levels.The latest research indicates that while overall injury prevention programs such as The II might reduce the incidence of trauma in amateur gamers, especially by reducing the incidence of knee injury. However, they will probably not benefit professional players or level. Instead, combining a more individualized approach (using a far greater emphasis on particular exercises determined by kinesiologic and diagnostic testing) with team sessions seems to be desirable. Additionally, it is important that gamers are 'on-board' with almost any program and take part regularly (at least twice weekly) to achieve all the potential advantages.
References
1.Br J Sports Med. 2002;36:354-9.
2.Injury Prevention. 2011;17(2):1-5.
3.Am J Sports Med. 2011 Jun;39(6):1226-32
4.Br J Sports Med. 2013 Aug;47(12):743-7.
5. Knee Surg Sports Traumatol Arthrosc 2010; 18:1798-1803.
6.J Orthop Sports Phys Ther 2010; 40:67-81
7.Br J Sports Med 2005; 39:542-546
8. Sports Med 2004; 34:681-695
9. Am J Sports Med 2002; 30:199-203.
10. Sports Med 2012;42:209-226
11. Br J Sports Med 2012; 46:112-117.
12.Am J Sports Med 2004; 32(suppl 1):S5-S16.
13. Am J Sports Med 2010; 38:2051-2057.
14. Am J Sports Med 2010; 38:1147-1153.
15. Br J Sports Med 2006; 40:767-772
16. Am J Sports Med 2013; 41:327-335
17. Am J Sports Med 2002; 30(5):652-9
18.Br J Sports Med 2012 Dec;46(16):1114-8
19. J Physiother 2013 Mar; 59(1):15-23
20. Clin J Sport Med 2013 Nov; 23(6):500-1
21. Sports Med 2013 Apr; 43(4):257-65
22.J Strength Cond Res 2013 Dec; 27(12):3275-85
23. J Muscles, Ligaments and Tendons Journal 2013; 324 3 (4): 324-330
24. J Bone & Joint Surgery 1936; 18:105-110.
25. Phys Ther Sport 2007; 8:14-21.
26.J Orthopaedic and Sports Physical Therapy 1981; 2:117-133
27. Magee DJ. Orthopedic Physical Assessment. 3rd ed. Philadelphia, PA: W.B. Sauders Company; 1997.
28. Spine 2003; 28: 1593-1600
29. Clinical Biomechanics 2004; 19:456-464
