




Chiropractor, Dr. Alexander Jimenez summarizes the anatomy and biomechanics of pectoralis minor, how tightness can create Injuries to the shoulder, and also powerful stretching and loosening procedures with this muscle…
The pectoralis minor (PMi) is a muscle located on the anterior chest wall which directly impacts movement an important consideration for proper movement that was scapulohumeral, of the scapula. It’s been suggested that tightness in the PMi can adversely affect scapula function(1-3), especially in limiting upward rotation, external rotation, and cerebral tilting(4), leading to shoulder injuries like impingement syndrome(1,5), and rotator cuff pathologies(6,7), internal impingement(7), glenohumeral instability(8) along with adhesive capsulitis(9).
Anatomy & Biomechanics
PMi is a wide triangular shaped muscle that originates from the second to fifth ribs as well as their costal cartilages through aponeurotic slips that are continuous with the facia covering the intercostal muscles(10). Within an old but comprehensive cadaver study, Anson discovered that 42 percent of those slips are connected from the second to the fifth ribs(10). However, this origin may be reduced to 3 or even to 2 ribs between the second to fifth ribs.Overall 91.5 percent of cadavers showed that the PMi arose from all or a few of the ribs between the fifth and the second. Cases where the source extended beyond the land of the next to the fifth ribs composed but 8.5 percent of the total amount.
From here the fibers course upwards and laterally and converge to insert onto the anteromedial and superior surface of the coracoid process. The PMi is found deep into the more superficial pectoralis major muscle, whereas the axillary blood vessels and brachial plexus lie posterior to the muscle (see Figure 1).

- Type 1 — happens when the entire PMi tendon passes through the superior margin of the process to fit on websites like one of the tubercles of the head, the coracoacromial ligament, the tendon, or the labrum.
- Type 2 — this variant is seen when a few portion of the thoracic has normal insertion into the process and another portion has insertion.
- Type 3 — happens when the muscle itself (as opposed to this tendon) inserts anomalously without attaching to the coracoid process.
PMi Function
The functions of the PMi (see Figure 2) have been to: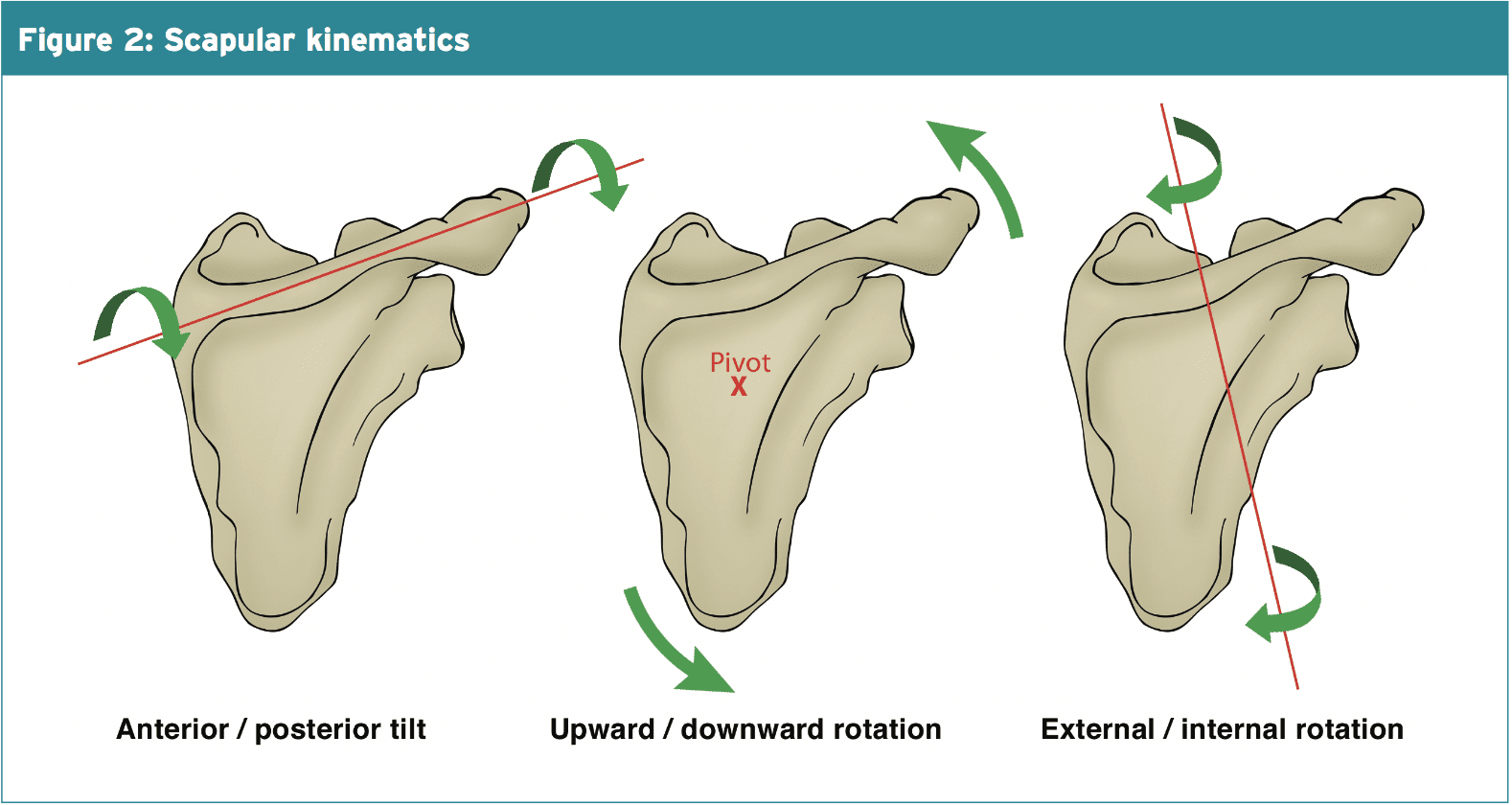
2. Downwardly rotate the scapula (along With rhomboids and the levator scapulae).
3. Anterior tilt the scapula (along with rhomboid and levator scapulae).
4. Depress the scapula (along with the Poor trapezius).
5. Rotate the scapula.
6. Help the inspiration muscles during breathing (because of its attachment on the rib cage).
Sporting/ training activities that involve these motions in the scapula (racquet sports, swimming, weight lifting etc) can theoretically result in overuse of the muscle, especially in the existence of training errors, poor technique or a rapid increase in training load, frequency and/ or length. Furthermore, the muscle can become constant reaching with one hand or shortened due to postural positions like sitting in a computer. These may all lead to tightness in the muscle, which will prevent complete scapular motion during overhead motions as it may limit upward bending and posterior tilt of the scapula, movements that are necessary for clearance of the acromian procedure away from the humeral head during arm elevation(3).

Injuries & Tightness In PMi
Due to its attachment on the coracoid Prevent upward rotation, elevation and posterior tilting of the scapula, which is required for shoulder elevation, and a shortening of PMi, process will result in anterior rotation of the scapula. Sahrmann (2002) has clarified a number of clinical syndromes that are associated with a shortening of PMi(15). These include; thoracic outlet syndrome, scapular winging and tilting syndrome, scapular abduction syndrome, scapular depression syndrome and scapular downward rotation syndrome.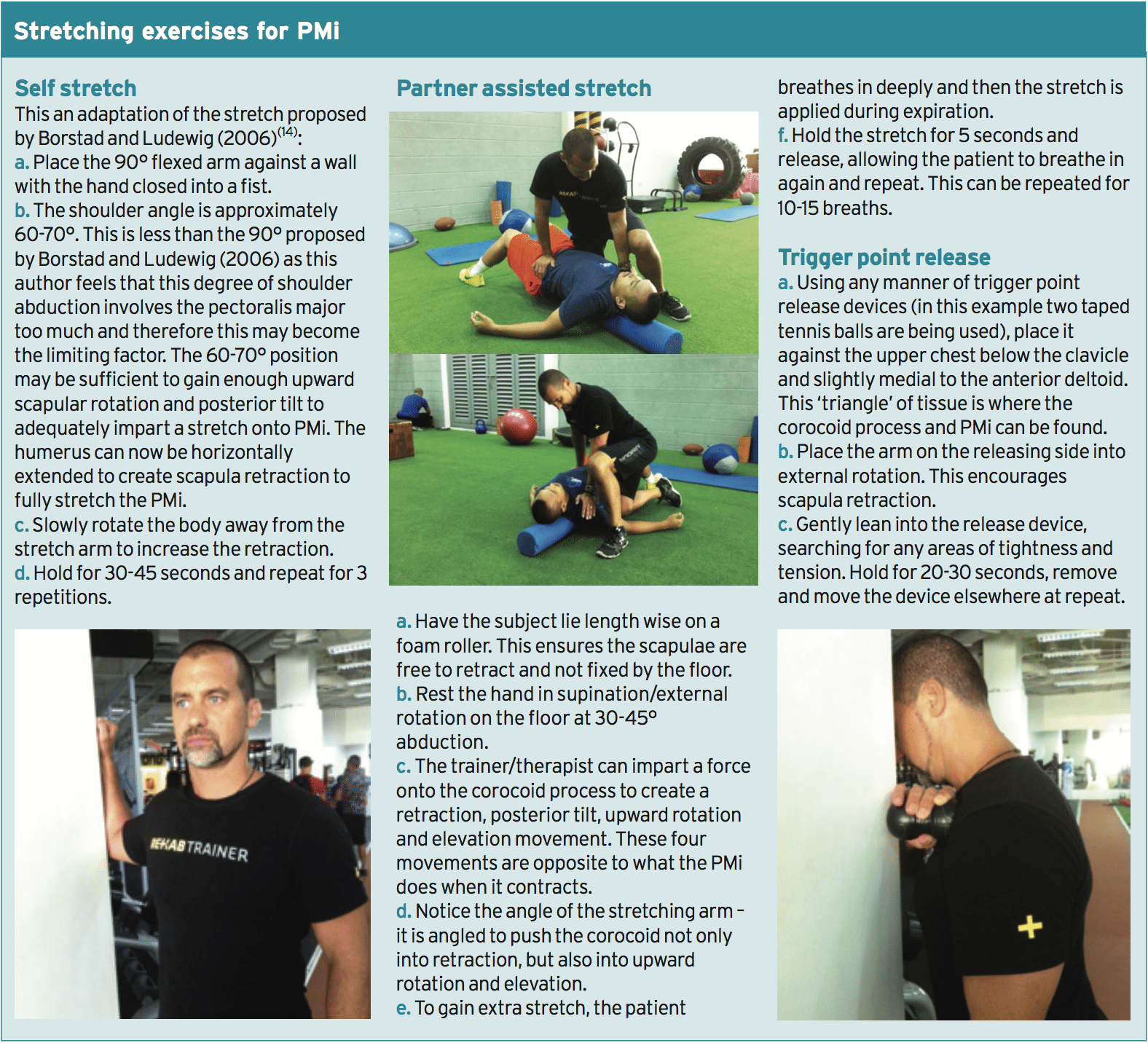
PMi Trigger Point Referral
Trigger points in the PMi can create pain in and around the shoulder. The quintessential reference point for whatever myofascial and trigger point related is Simons and Travell (1999)(17). They explain a pain referral pattern of PMi as pain over the anterior deltoid region and spilling over into the subclavicular and pectoral areas. The pain can extend down the medial aspect of the arm, forearm, and into the ulnar supply of the third and their hand, fourth, and fifth digits. Lawson et al (2011) introduced a case study on how PMi trigger points generated pain like angina in a cross country skier(18).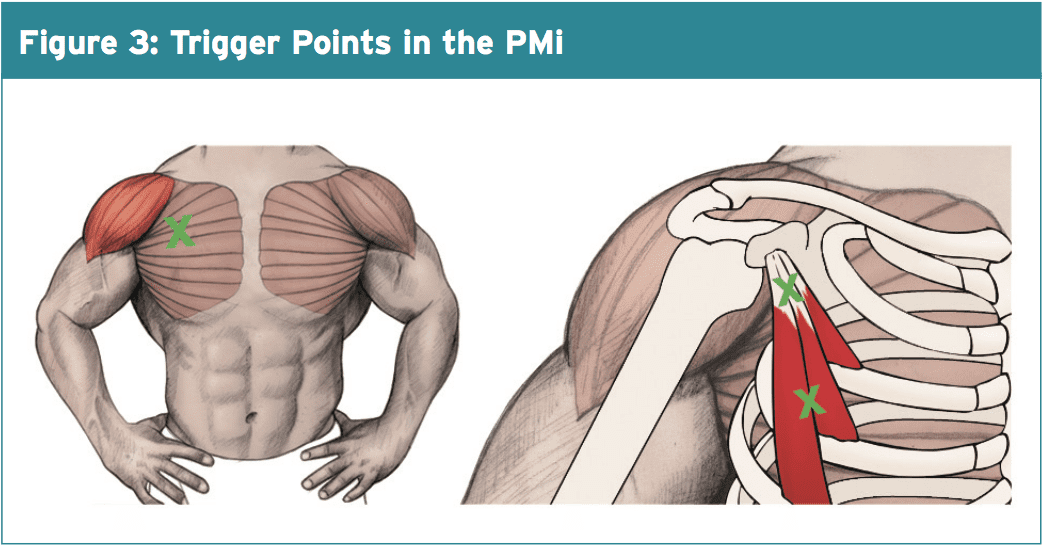
Summary
The PMi has been identified as a muscle that is implicated in scapula dysfunction and following shoulder pathologies. Tightness in the muscle can limit full Scapula upward rotation elevation — movements which are required to Enable clearance of the acromian Process away from the humeral head in elevation rankings. Stretching exercises for the PMI have been provided to Lengthen and decrease tone problematic muscle.References
1. Phys Ther. 2000; 80(3):276-291
2. Sports Medicine and Arthroscopy Review. 2012; 20(1):39
3. J Orthop Sports Phys Ther. 2005; 35(4):227-238
4. Phys Ther. 2009; 89(4):333-341
5. J Orthop Res 2001; 19(6):1192-1198
6. J Shoulder Elbow Surg. 2005;14(1 SupplS):58S-64S
7. J Orthop Sports Phys Ther. 2006; 36(7):485-494
8.Am J Sports Med. 2007; 35(8):1361-1370
9. J Biomech. 2008; 41(2):326-332
10. J.Anat. 1938; 72(4); 629-630
11. Korean J Radiol. 2014;15(6):764-770
12. Int J Sports Physical Ther. 2013; 8(1);25-33
13. BMC Musculoskeletal Disorders 2007; 8:64
14. J Shoulder Elbow Surg. 2006; 15(3):324-330
15. Sahrmann S: Diagnosis and treatment of movement impairment syndromes. London: Mosby; 2002
16. Br J Sports Med. 2007 Aug;41(8):e11
17. Simons DG, Travell JG, Simons LS. Travell & Simons’ myofascial pain and dysfunction. The trigger point manual volume 1. Upper Half of Body. 2nd ed. Baltimore, MD: Williams & Wilkins; 1999
18. J Chiropractic Med 2011; 10, 173–178
19. J Can Chiropr Assoc. 2012 Dec;56(4):311-5
