




Chiropractor, Dr. Alexander Jimenez takes a look at a often injured shoulder muscle…
The supraspinatus muscle is one of the four rotator cuff muscles of the shoulder. It originates in the central area of the supraspinatus fossa of the scapula then courses laterally to cross the joint capsule of the shoulder and attaches onto it it then passes under the acromion and the coracoacromial ligament and fans out and inserts to the lateral and superior aspects of the greater tuberosity of the humerus. The fascia supraspinata covers the superficial region of the muscle. Superiorly it contacts the deltoid and trapezius muscles, whereas the deep fascia attaches to the joint capsule.
The supraspinatus has a function in the initiating active shoulder abduction and providing abduction torque (especially in the first 30 levels of shoulder abduction) along with the more powerful deltoid, and it also plays a role in depressing the humeral head and centralizing the humeral head in the glenoid through abduction/flexion moves. It’s been proven in biomechanical studies which during busy shoulder abduction, the pressure vector made by the supraspinatus (which acts as a humeral head compressor and depressor) as well as the anterior/middle deltoids (humeral head elevators) creates a force couple whereby the humeral head stays centred in glenoid fossa. In the event of a weakened supraspinatus, greater deltoid activity ensues and this is going to bring about a superior shear of the humeral head with regard to the glenoid(2,3). This may then create the superior rim and a impingement between the humeral head, acromian procedure and arch.

Finally, the supraspinatus may contribute to internal rotation torque manufacturing and external rotation; however, that is varied upon flexion/extension angles of the shoulder and the abduction. For the most part, it contributes little towards pure rotation torque at the glenohumeral joint.
Incidence Of Injury
Injury has a high prevalence From the population. It’s very common in the older population which suggests that progressive degeneration is a element in developing a full thickness tear in the tendon. Research has postulated that in individuals under the age of 40 the prevalence is a small 4 percent; however, in those ages 60 and above the incidence rapidly increases to 54 percent(4).Even in patients with no shoulder pain, The incidence of rotator cuff injury is comparatively high. Tempelhof et al (1999) found that even in asymptomatic people, ultrasound finding demonstrated that at the 50-59 age group 13\% had tears, at the 60-69 age category 20 percent, at the 70-79 age group 31\% and at the older 80+ age group 51 percent of asymptomatic shoulders had tears in the rotator cuff (5).
Yamamoto et al (2010)(6)) supports this Predisposition by indicating arm dominance as well as that and preceding shoulder trauma, era was in creating a rotator cuff tear, another risk factor. What they found was that the incidence of rotator cuff tears increased linearly with age (0 percent in the 20s group, 2.5\% at the 30s group all the way around 50 percent in the 80s group). Interestingly, 17\% of issues with rotator cuff tears complained of no symptoms. In essence, many older individuals may have a true partial/full thickness tear of the supraspinatus and be completely unaware that the injury exists(6).
Research shows that from the Lack of a supraspinatus (due to a complete thickness tear of the supraspinatus tendon), the humeral head will migrate superiorly and abut the acromian, highlighting the value of the supraspinatus in centering the humeral head in the glenoid and preventing a superior migration of the humeral head(7,8,9,10). Repeated exceptional migration of the humeral head will produce an impingement scenario and repeated episodes of impingement will result in breakdown and damage to the subacromial bursa, arthritic changes in and around the glenoid and humeral head and acromioclavicular joint fluctuations in the inferior part of the joint.
From the younger athletic population, true Partial/full thickness tears are rare unless it’s associated with a serious shoulder injury such as a dislocation or when the arm is forcefully whilst a scenario which might occur in contact sports such as rugby and NFL, in an abducted position. Injury to the supraspinatus involves phase tendinopathy which might result in an supraspinatus tendon due to mechanical overload. Finally, trigger factors that are active can develop in the supraspinatus that can create searing pain throughout the deltoid and upper arm.
Mechanism Of Injury
Interestingly in the population that is elderly, Injuries to the supraspinatus may come from activities like lifting a heavy bag or holding a puppy on a lead and the puppy runs or stops, leading to a tug onto the arm. From the younger people, direct injury to the supraspinatus may appear due to a trauma episode such as fall onto an outstretched hand, dislocating a shoulder, sustaining a solid adduction force on a flexed/ abducted shoulder or falling off a bicycle and retaining hold of the handles. It might come from exercise like swimming pool, tennis and other sports that are overhead through overload movements such as Olympic-type lifting, repetitive and powerlifting trauma.The supraspinatus is a tendon that is Exposed to forces within an extended time period, highlighting the prevalence of tears from the people. Neer (1983)(11) has been the first to describe the three phases of rotator cuff disease, particularly the changes found from the supraspinatus. But he didn’t elucidate if the trigger was tendon degeneration or mechanical impingement or a combination of the two. Stage I occurs in patients < 25 years using oedema and haemorrhage of the tendon and bursa. Period II involved inflammation and fibrosis of the rotator cuff in patients aged between 25 and 40 years old. Phase III involves tearing of the rotator cuff, either partial or full- depth, and occurs in patients 40 years old(11).
It is possible that some small Supraspinatus tears can heal or become smaller; however, Yamanaka and Matsumoto (1994) revealed that roughly 53\% grow further and 28\% might advance to full thickness tears. It is thought that full thickness tears do not heal due to poor vascularisation within the tendon(12).
Presenting Symptoms & Signs
SubjectiveThe more serious thickness tears or the patient with a grade supraspinatus injury will complain of antero-lateral shoulder pain that is made worse by any action where the arm is raised up to 90 degrees of abduction or flexion. Sleeping on the shoulder might be painful. Holding weights and lifting like hanging towels on a clothes 14, things might turn out to be rather painful and functionally impossible to perform. As emphasized previously, many incidences of supraspinatus pathology can in reality be curable and painless.
Objective
Palpation
The individual will usually be tender to Palpate in and around beneath the acromian process the head.
Energetic Movements
Abduction moves and full flexion will Most probably be hard and painful to completely execute based on severity of the injury. Whereby the pain will be present from 80-160 levels of abduction, stage 1-type accidents will have an arc of pain throughout abduction. In more serious partial thickness and full thickness tears, complete abduction could be impossible to perform because of an inability of the muscle to commence abduction, or the quality of the movement might be quite poor whereby the individual elevates or ‘hitches’ the scapula to commence abduction.
The test for supraspinatus/rotator Cuff impingement is the Neer test first Clarified in 1972. In this evaluation the patient is Asked to bend the shoulder Whilst the holds stable the scapular examiner. Typically the pain is felt at Around 120 levels of shoulder flexion(13). Jia et al (2011) looked in the internal Construction of the shoulder an Arthroscope and found that in most cases The rotator cuff (supraspinatus contained) contacted the superior glenoid rim. These findings Patients believed The pain when assessed clinically. Therefore accidents to the supraspinatus May present as pain in the anterior/lateral Once the arm is flexed to 120, shoulder Levels(14).

Resisted Muscle Tests
Patients with grade supraspinatus pathology will test normal with the vast majority of resisted spinning movements and abduction moves. The more serious tendon lesions such as partial/full tears will usually pose as weakness in external rotation and abduction ( with or without pain). Muscle testing to the supraspinatus can be accomplished using an ’empty can’ or ‘complete can’ test.However, a lot of studies since have shown that the ’empty can’ position is not necessarily the ideal position for exercising and testing for supraspinatus with no extra curricular activation. The scientific basis for this debate has stemmed from the many EMG research studies in the past decade which have quantified supraspinatus activity. For example, Blackburn et al (1990) indicates the contrary movement for testing/strengthening supraspinatus — that the ‘full can’ movement. That is equal to the ’empty may’ the arm has been retained in external rotation as opposed to internal rotation. This elucidates the identical degree of supraspinatus activity, without the superior shear effect of the deltoid(16).
Testing places and exercises that produce higher degrees of activity in regard to supraspinatus activity may be counter-productive in patients with weakness of the rotator cuff, shoulder pain, and stabilization that is ineffective. As a result, the may place may give false positives because the source of pain may be direct impingement of the subacromial structures as a result of superior migration of the head as a result of deltoid contraction.
From an anatomical and biomechanical standpoint, the full can exercise also might be the most beneficial position to both test and exercise and provoke the smallest amount of pain due to the least quantity of humeral head outstanding migration and increased minute arm of the supraspinatus muscle in this place compared with the empty can place.
Rehabilitation Of Supraspinatus Injuries
Partial thickness tears and early stage supraspinatus accidents may do well when managed. Larger partial thickness tears and total thickness tears will need to be properly managed to acquire a favourable outcome. For the paper’s purposes, the discussion will focus on the conservatively managed supraspinatus injury.It appears that the best exercises to the supraspinatus would elicit the best quantity of activity that is supraspinatus while reducing particularly the deltoid, the muscle activity. Boettcher et al (2009)(17) studied this specific phenomenon when they analyzed that the EMG activity (15 subjects) of a number of shoulder muscles including supraspinatus, infraspinatus and deltoids whilst performing these motions: full can moves, empty may move, prone elevation, external rotation in 0 degrees abduction and prone external rotation positions. The exercises were performed together with the scapular in a retracted position. Each of of the exercises were stored isometrically for five minutes, using a one-second build-up phase, a grip along with a discharge phase.
They sought to appear at which ones recruited deltoids at the least but also which exercises greatest supraspinatus that was triggered. What they found was that each of five selected exercises triggered the supraspinatus to a degree, and specifically there was no difference between ‘can’ and ’empty can’ moves. They discovered more prone activated muscles within this order of magnitude: posterior deltoid anterior. The rotation at 0 degrees and the prone external spinning activated infraspinatus the most, however, supraspinatus action still out performed all the deltoids; and more importantly, both of these exercises also recruited far less deltoid than the ‘full can’ and ’empty may’ moves. They contended that the best exercise to get supraspinatus was that the exercises that incorporate external rotation rather than the ‘can’ and ‘can’ movements. The researchers assert that exercises need to be selected as it has a superior migratory influence in the head, that restrict deltoidscausing impingement of the supraspinatus against the coracoacromial and acromian space.
Reinold et al (2007)(18) conducted a similar study on comparing the ’empty can’, ‘ ‘full may’ and ‘inclined full can’ moves and quantifying EMG activity from the middle deltoid, posterior deltoid and supraspinatus muscles. What they discovered was that even though all three exercises produced comparable amounts of activity that is supraspinatus, the can exercise generated significantly less action of the deltoid muscles and could possibly be considered to be the optimal place to recruit the supraspinatus muscle for testing and rehabilitation. The empty may exercise could be a good exercise and also the full that is more likely can exercise may be a great exercise. These findings have been supported by Lee et al (2014)(19) who revealed using PET/CT imaging the ‘full can’ position was more effective as an exercise for supraspinatus without predominant deltoid action. Ultimately, Escamilla et al (2009)(20) suggests that scapular protraction and scapular anterior tilt, both of which reduce subacromial space width and increase impingement hazard, are higher when performing scaption moves with inner rotation (’empty can’) compared with scaption with external rotation (‘total may’).
Therefore it appears that the ‘safest’ exercises to recruit supraspinatus and also minimise the deltoid are the ‘full can position’ and also the ‘external that is prone rotation’ exercise. These two exercises may form the basis of applications that are re-strengthening that are supraspinatus. These exercises have been described below. Furthermore, supraspinatus function that is effective will only be evident with a scapula base that is functioning and strong. Immediate exercises to retrain the anterior and strengthen and lower trapezius will be required to allow scapular positioning.
The Exercises
1. Full Can Exercise
Stand holding small dumb-bells (2.5pound women , up to 5kg for guys) or rubber tubing. Begin with the hands by both sides along with the horn turned outwards. Lift the arm to abduction whilst retaining the angle of the arm around 30 degrees to the frontal plane. Initially if the shoulder is painful the scope may be limited to 30 levels; nonetheless, as pain and strength boost they may move the arm to further positions of abduction.Work on three sets of 15-20 repetitions.
2. Prone Spinning exercise
Lie begin with the arm dangling down along with the arm at 90 degrees abduction and face down. Gently retract and depress the scapula. Slowly raise the arm to external rotation whilst attempting to keep up the scapula position. Perform three sets of 15-20repetitions.3. Scapular Wall Slides
As per the graphic below, begin with the forearms in contact. Slide the arms up the wall slowly externally rotating forearms on the way upward. This will produce scapula spinning and protraction to activate the anterior, a muscle at the control of scapula motion and thus rotator cuff function in overhead sports.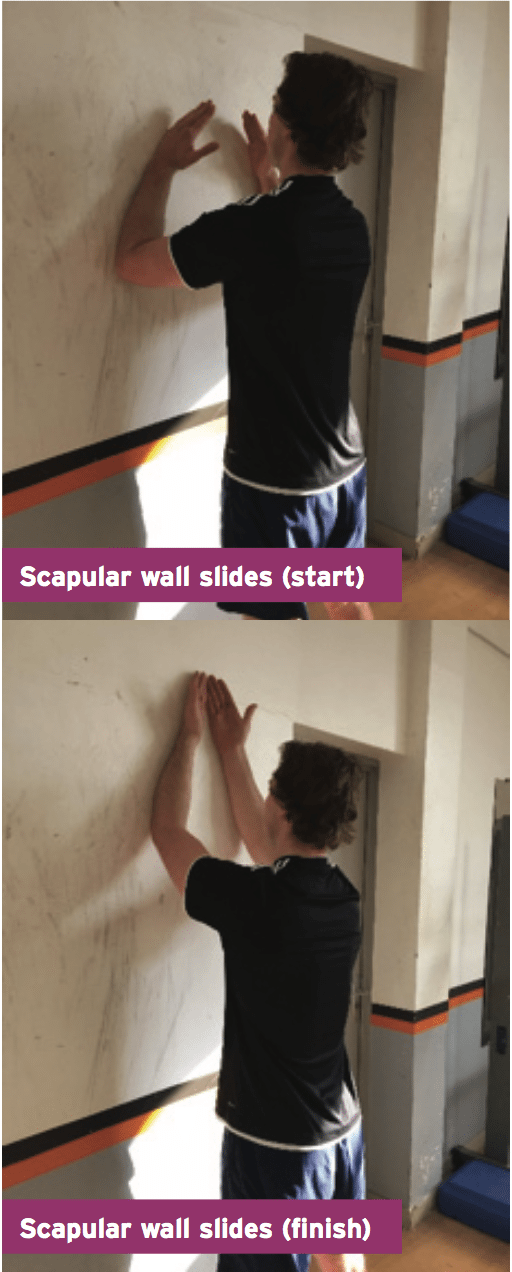
4. Lower Trapezius Setting
The most easy way to perform this and also to teach this as an exercise is to do this drill on a lat pulldown machine. Use only light resistance such as 3-4 plates on the pulldown machine. Seated with the hands gripping the lat pulldown bar, gradually draw on the scapula down and in (retract and depress). Hold for a quick 1-2 seconds and then repeat for two sets of 15 reps.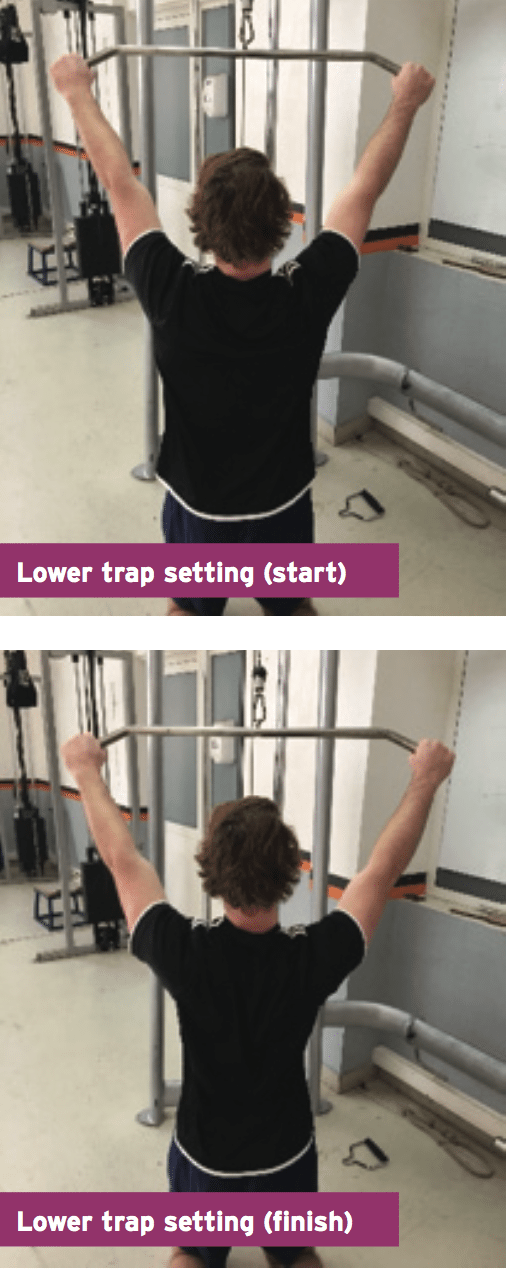
Conclusion
Research shows that the supraspinatus plays an important part in the shoulder as it centers the humeral head into the movements of the arm/ shoulder. Dysfunction in this muscle may lead to excess of the head which might be a precursor to shoulder instabilities and the more shoulder impingements. Injuries to the supraspinatus are typical as well as also the cause of rotator cuff disorder especially in the older athlete. This article has offered a framework for treatment and evaluation of dysfunction.References
1. Journal of Ultrasound 2010; 13. 179-187.
2. Biomechanics of the shoulder. In: Rockwood CA, Matsen FA, eds. The Shoulder. Philadelphia, PA: WB Saunders; 1998:233–276.
3. Clin Orthop Relat Res 1978; 135. 165–170
4. J Bone and Joint Surgery (Am) 1985; 77-A. 10-15.
5. J Shoulder and Elbow Surgery 1999; 8(4). 296-299.
6. J Shoulder and Elbow Surgery 2010; 19(1). 116-120.
7. Clin. Imaging 1995; 19. 8–11.
8. Clin. Biomech 2006; 21. 942–949.
9. J. Shoulder Elbow Surg 2003;. 12. 179–184.
10. Clinical Biomechanics 2007; 22. 645–651
11. Clin Orthop 1983. 173; 70-77.
12. Clin Orthop 1994; 708. Pp 68-73.
13. J Bone Joint Surgery (Am) 1977: 54. 41-50
14. Clin Orthop Relat Res 2011; 469: 813–818
15. Am J Sports Med 1982;10:336–339.
16. Athl Train J Natl Athl Train Assoc 1990; 25:40–45.
17. Sci. Sports Exerc 2009. 41(11); 1979-1983.
18. J Athl Train 2007; 42(4): 464–469
19. J Orthop Surg Res 2014; 9(1): 85.
20. Sports Med 2009. 39(8). 663-685.
