




Although golf is regarded by many as a ‘gentle’ game, the threat of back pain among its practitioners Is surprisingly high. Chiropractor, Dr. Alexander Jimenez explains the kinematics resulting in back pain in golfers…
Golf’s leisurely nature clubs makes it popular with older adults who might be unable or reluctant to take a sport, where the dangers of injury are perceived as far higher. However, the quantity of physical activity required to play golf remains adequate to provide health benefits.
Surprisingly, however, the reality of golf and injury risk is somewhat different. While a properly executed golf swing might not seem particularly stressful, a number of biomechanical studies have shown that many joints and limbs are in reality moving at high velocity and during extreme ranges of motion (ROM)(1-3), which makes them vulnerable to trauma. The successful implementation of the golf swing takes a high degree of coordination, requiring many hours of training during which these movements are repeated hundreds of times to make things worse. Insert the fact that the golfers using poor swing actions are the most likely to be practicing and that faulty swing mechanics are likely to lead to an accident and you have a recipe for injury.
Prevalence Of Injury
Putting aside of being struck by a golf club, ball, a golf cart or perhaps lightning(!) Related to golf practice are likely to afflict the trunk and upper body. Studies show that elbow injuries and hand/wrist harms are quite common, affecting approximately 13-20percent and 25-30percent of golfers . Shoulder injuries are rather common, affecting around 8-18percent of amateur golfers. The corresponding figures for professional golfers tend to be considerably lower, however(4-7).The incidence of low back pain (LBP) One of golfers by contrast is a somewhat more prevalent, and is proven to influence amateurs and professionals alike, regardless of skill levels(8). Epidemiological studies have revealed that low back conditions account for roughly 25% of all golfing injuries(9,10) even though prevalence rates as large as 54 percent (28) are reported(11). In a 2009 literature review, colleagues and Cabri reported that trauma to the back signified the most common complaint experienced by both amateur and professional golf players.
Another study researched 196 Golfers who had only taken up the game(12). While 25\% suffered pain back during the analysis period, the majority of those participants were unaware that playing golf was linked to their LBP. The authors concluded that golf may aggravate pain due to the forceful nature of the motions associated with playing and practicing.
Benefits OF Chiropractic For Golfers
Demands Of The Swing
To understand how something Seemingly benign as golf can cause a high prevalence of lower back pain, so it helps to appreciate the biomechanics of the swing (see Figure 1). The golf swing involves a slow deliberate turning of the trunk from the target (the backswing) followed by a strong rotation of the trunk towards the goal on the downswing. Although there are other spinal movements present throughout the swing motion, the axial twisting forces are especially notable because this type of writhing has been identified as a substantial risk factor for low back injury disorders in occupational settings(13).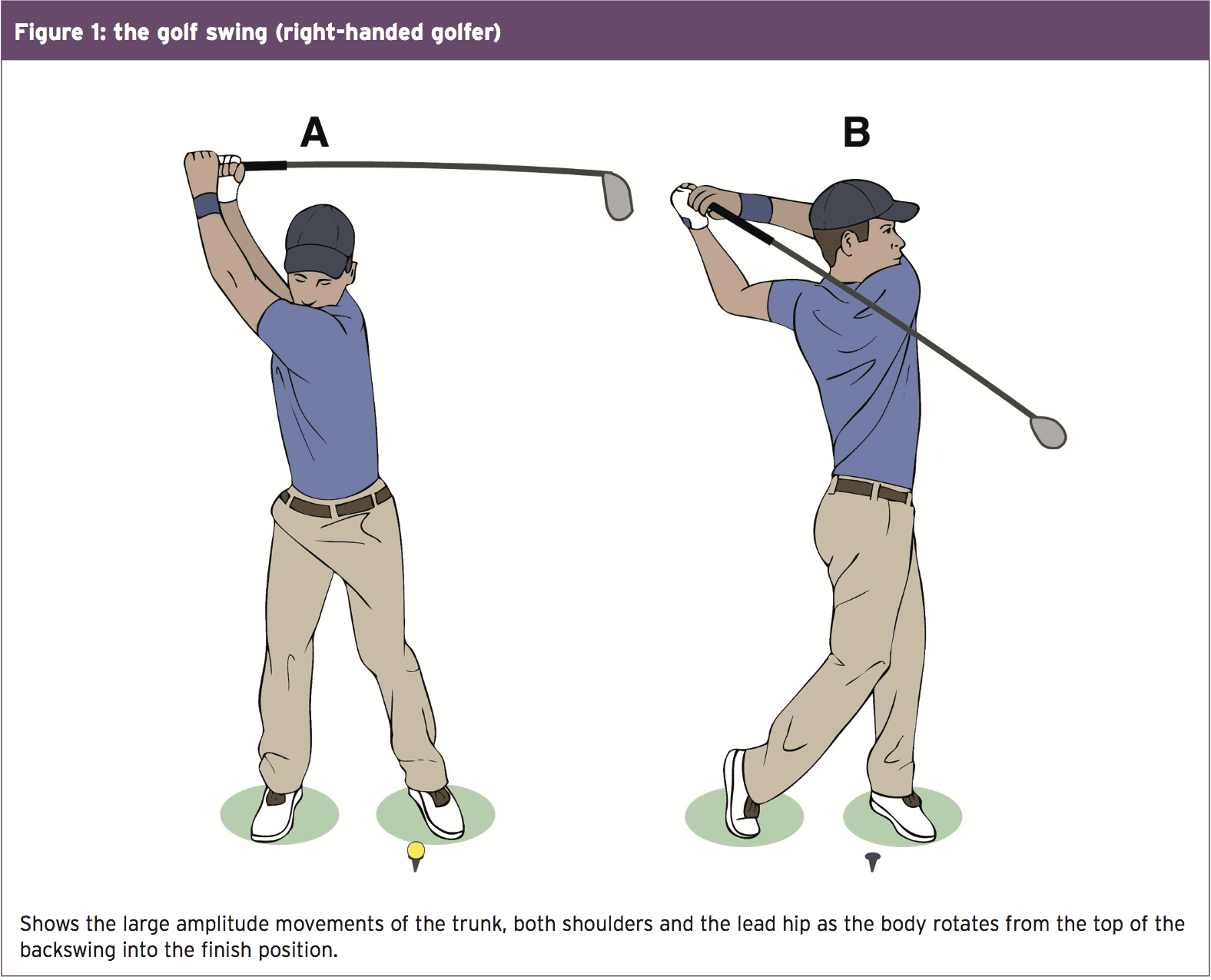
Studies investigating the axial forces at Play throughout the swing motion have produced some startling findings. Among the first studies looked at forces on the lower back during a full golf swing whilst using a five iron — especially the compressive, shear, lateral- bending and rotational loads over the L3/4 segment of the thoracic spine(14). Kinematic, kinetic and surface EMG data was collected from four pro golfers and four amateur. Shear loads were high but were higher averaging 596 Newtons of power 329 Newtons from the pros. Loading on the other hand has been greater averaging nearly 7,600 Newtons versus 6,100 Newtons in the amateurs.
To place these loads in View, consider that forces are generated by the swing of an expert golfer around of an amateur around six times bodyweight and eight times his/her bodyweight. Think about that spinal compression forces in a runner are about three times body fat, and you may start to appreciate the issue. It’s also worth noting that cadaveric studies have proven disc prolapse to occur with compressive lots of approximately 5,500 Newtons, which explains why the swing motion can boost the risk of a serious low back injury(15).
Despite the risk of acute low back injury as a result of the swing report the onset of LBP.
Insidious LBP is thought to happen as a Consequence of loading as a result of The mixture of magnitude Forces together with a high Frequency of swing repetitions. Studies Reveal that elite golfers consistently Suffer LBP during golfing activities tend To get a greater frequency of swing Repetitions (ie spend more time playing And practicing) than symptom-free Golfers(16). Cumulative loading probably Clarifies why elite players identify overuse Rather than a traumatic event because the trigger Of the LBP(17).
Asymmetry & LBP
As we could see in Figure 1, a comparatively slow backswing followed with a downswing and follow-through produces an asymmetrical back rotational velocity, leading involving the trail and lead sides. Indeed, studies show that LBP predominantly happens on the road side — ie the right side of a right-handed golfer and radiological analyses of elite gamers have demonstrated a significantly higher rate of path side vertebral body and facet joint arthritic change than age-matched control subjects(11).Other researchers have also noticed that both left axial rotation velocity and appropriate side-bending angles onto the downswing reached peak values almost simultaneously and after ball effect, coinciding with the point where the majority of players in their analysis document experiencing LBP(18). The implication is that a large amount of side bend angle combined throughout the impact stage damages by creating intervertebral shear, the thoracic spine. This motion is possibly harmful since it is resisted by disk strength instead of bony architecture, thereby resulting in injury and painon the road side.
One approach to decrease lateral shear is to decrease right-side bending (at a right- handed golfer). Studies reveal that elite players with LBP tend to deal with the ball with more spinal flexion — ie they slouch longer and use more side-bend throughout the swing compared to healthy golfers(19). The good news for golfers is when setting around the ball that decreasing the amount of side-bend that is right on the downswing may be as straightforward as using position. In addition, it is important to notice longer clubs may help in this respect and that bending promotes.
The ‘X’ Factor
In a bid to hit the ball further and harder, a backswing, which in theory at least allows time for maximum power to be generated before ball contact is developed by many golfers. Backswing creates axial loading in the spine. Once the pelvis begins rotating towards the target a fraction prior to the acromion or shoulder line, this is particularly true during the initial stage of the downswing. The concept is to create the maximum ‘X’ factor stretch — defined from the transverse plane between a line connecting the right and left anterior superior iliac spines and a second line drawn through the acromion processes. A player can increase this ‘X’ variable stretch by up to 19% throughout the first stage of the downswing.The problem, obviously, is that this stretch introduces higher loadings to the backbone. A supra-maximal or over-rotation twisting of the trunk when increases the risk of spinal irritation and subsequent LBP. Moreover, many golfers are not able to replicate this amount of rotational stretch in the practice when asked to do this from a position in a moderate rate. It has led some investigators to question if the loading can be reduced.
One study found that reducing the comparative amount of spinal distress or torsion by increasing the range of hip turn during the backswing could assist in cases of golfing-related LBP(20). In another study, researchers asked whether an intense backswing was essential(21). The researchers investigated the effects of using a backswing on ball- club-head rate and contact accuracy. The results showed that restricting the backswing by nearly 20\% (thereby decreasing spinal loading) had no adverse impact on overall swing operation.
These and other outcomes have led some investigators to suggest that golfers with LBP adopt a more ‘classic’ golf swing — as being used in an earlier age of the match. A reduced X factor, which decreases the following and torque stress on the lumbar spine is incorporated by the swing. This is achieved by allowing the lead heel (ie left heel in a right-handed golfer) to lift during the backswing to allow the pelvis (and not just the shoulders) to flip off from the goal.
Getting To The Core
Considering the role of trunk musculature in generating the swing movement (equally downswing and backswing), it’s unsurprising that investigators have investigated whether core muscle dysfunction is implicated in golf-related LBP. Some studies do suggest that golfers with LBP appear to trigger their trunk muscles to symptom-free golfers, and it’s likely that over time, these differences contribute to decreased back muscle strength and endurance.As an example, one study found that the beginning times of major bursts of activity from a number of the abdominal muscles were delayed in the golfers afflicted LBP(22). Specifically, the direct external oblique (left in right-handed golfers) has been activated significantly later throughout the backswing from the golfers with LBP when compared to asymptomatic controls. Another study looked at EMG activity from the abdominal and back muscles of golfers with and without LBP, also discovered that highly skilled players tended to show reduced erector spinae action near the top of the backswing and at ball impact(23).
A small number of studies have compared back muscle endurance in golfers with and without LBP. For instance one study (51) investigated the total time golfers with and without LBP can maintain an isometric transverse abdominis regeneration and found that healthy golfers could keep the static contraction for substantially more than the golfers with LBP(24). This is relevant because transverse abdominis is known to be very important for shielding the thoracic spine by tensioning the thoracolumbar fascia(25).
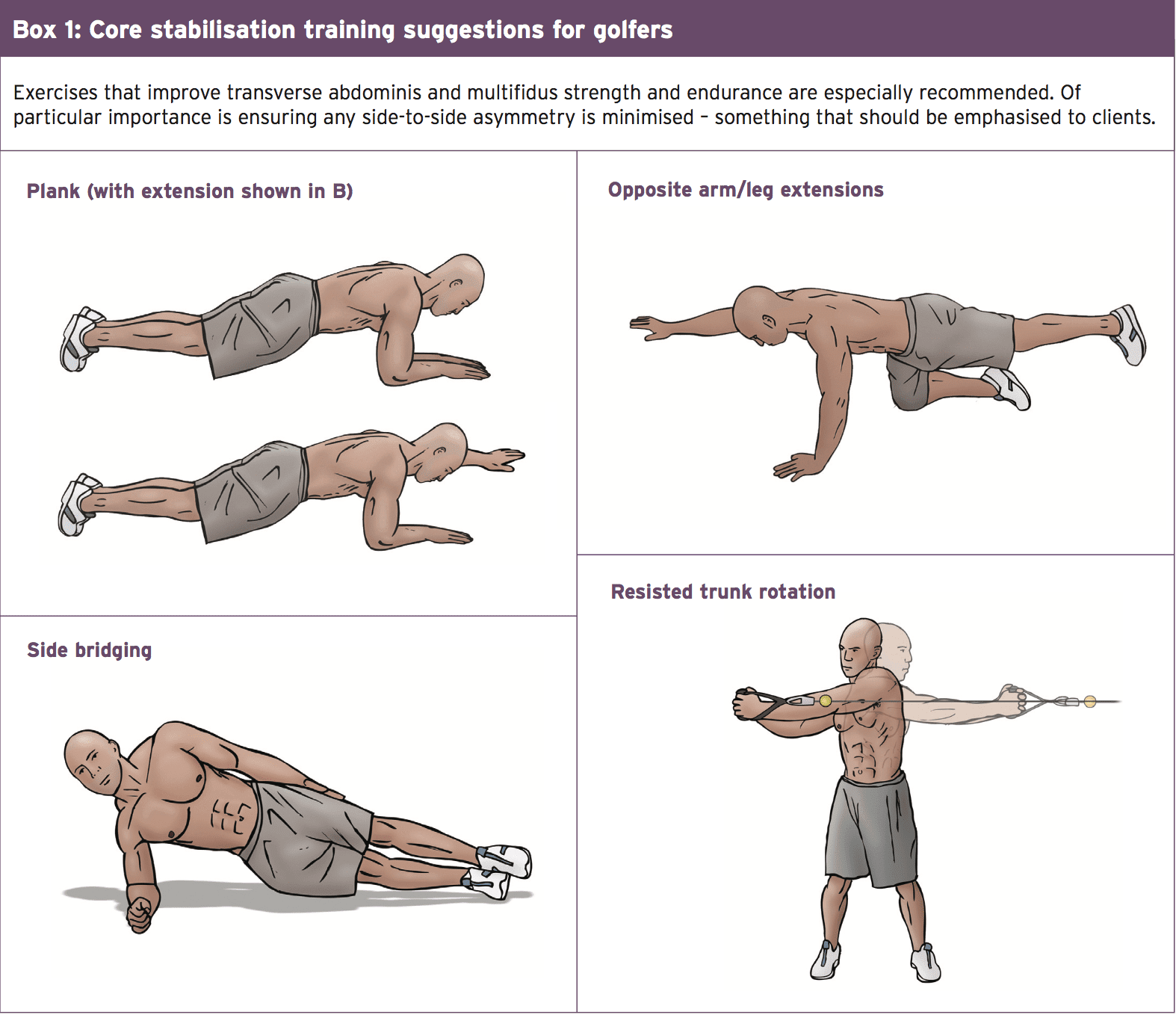
Another study found that isometric trunk extensor (eg erector spinae) holding times for golfers with LBP was considerably lower than values reported by healthy areas(26), along with an Australian analysis on trainee golf professionals found that golfers using a path negative (ie right side to get a right-handed golfer) shortage of 12.5 seconds on the static side- bridge endurance evaluation reported more frequent episodes of moderate to acute LBP(27). Further evidence indicates that elite golfers have a tendency to have greater axial rotation strength in the way they generally swing a golf club (ie to the left for a right-handed player) and that this asymmetry or imbalance is very likely to be more pronounced in golfers with LBP(28). Together, these findings imply that most golfers, but particularly those vulnerable to LBP should execute some regular core stabilization training exercise (see Box 1).
Summary & Recommendations
It’s more than likely that the regular custom of his/her sport is going to be a major element when a golfer poses with low back pain. Besides the typical treatment modalities for LBP, it is useful for clinicians to understand how the kinematics of golfing could result in LBP and what practical recommendations regarding golfing clinic could be made to individuals in order to accelerate recovery and reduce the risk of re-injury. Box 2 outlines these recommendations.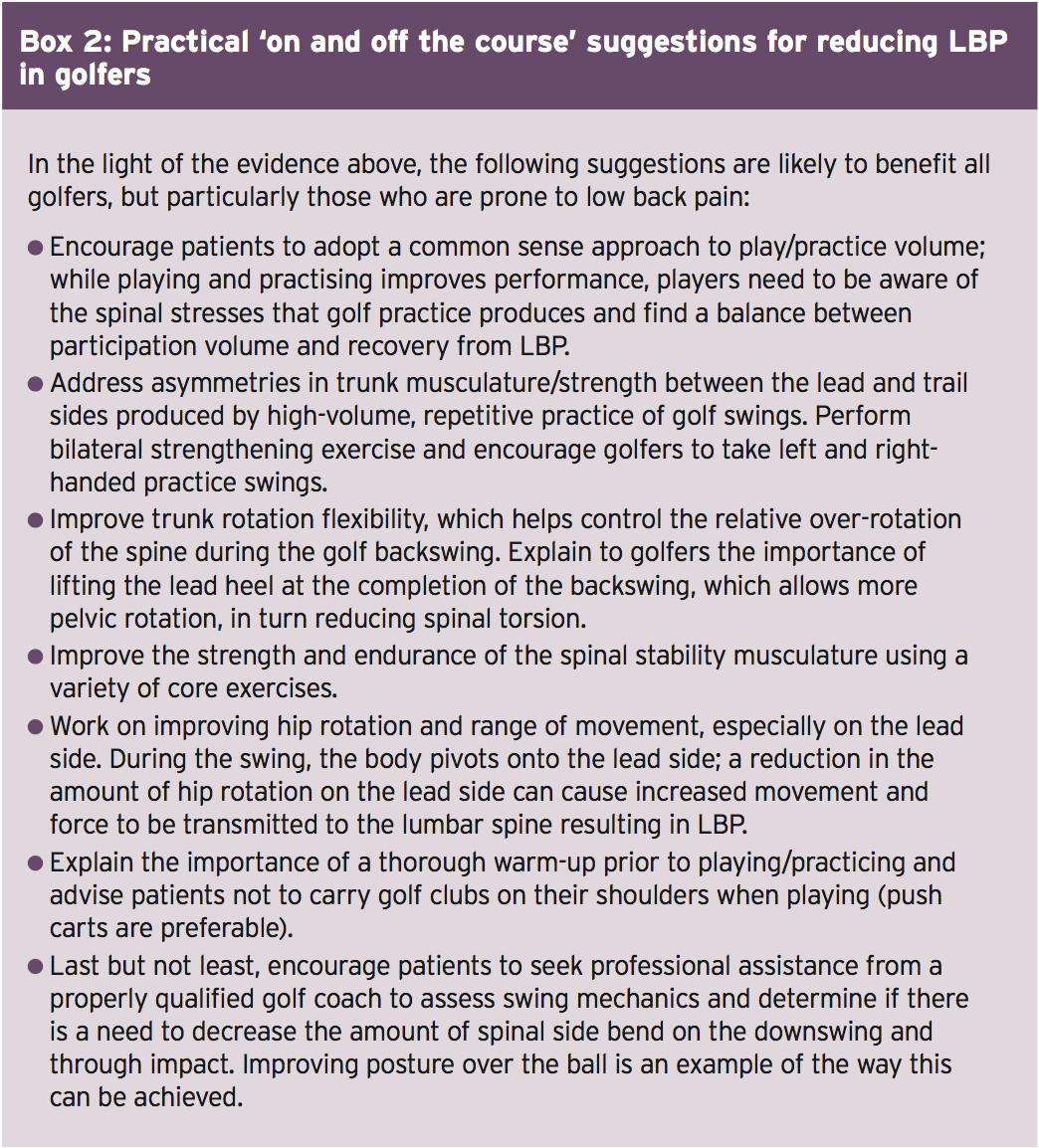
References
1. J Appl Biomech. 2002;18:366–73
2. Sports Med.2005;35(5):429–49
3. J Appl Biomech. 2011;27(3):242–51
4. Am J Sp Med. 2003;31:438–443
5. Phys Sports Med. 1990;18:122–26
6. Br J Sports Med. 1992;26:63–5
7. Phys Sports Med. 1982;10:64–70
8. Clin Sports Med.1996;15(1):1–7
9. Br J Sports Med. 1992;26(1):63–5
10. McNicholas MJ, Neilsen A, Knill-Jones RP. Golf injuries in Scotland. Human Kinetics; 1999
11. Low back injury in elite and professional golfers: an epidemiologic and radiographic study. Champaign, IL: Human Kinetics; 1999
12. Am J Sports Med. 1996;24(5):659–64
13. Ergonomics. 1995;38(2):377–410
14. Biomechanical analysis of the golfer’s back. Cochran AJ editor. London: E and FN SPON; 1990
15. Mechanics of the intervertebral disc. Ghosh P editor. Boca Raton (FL): CRC Press; 1988
16. J Sports Sci. 2002;20(8):599–605
17. Phys Sportsmed. 1982;10:64–70
18. Morgan D, Sugaya H, Banks S. A new twist on golf kinematics and low back injuries. South Carolina: Clemson University; 1997
19. J Sports Sci. 2002;20(8):599–605
20. Med Sci Sports Exerc. 2000;32(10):1667–73
21. J Manipulative Physiol Ther. 2001;24(9):569–75
22. Med Sci Sports Exerc. 2001;33(10):1647–54
23. J Sci Med Sport. 2008;11(2):174–81
24. J Man Manip Ther . 2000;8:162–74
25. Phys Ther. 1997;77(2):132–42
26. Spine (Phila Pa 1976). 2001;26(16):E361–6
27. Phys Ther Sport . 2005;6:122–30
28. N Am J Sports Phys Ther. 2006;1(2):80–9
