




Chiropractor, Dr. Alexander Jimenez looks at the treatment options for tendon injuries based on the inflammation & degeneration paradigm strategy.
Tendons are bands of tough connective tissue at the ends of muscles that transfer forces between bones and muscles to move joints and maintain posture. They store kinetic energy, absorb shock, and assist in proprioception. To survive the fantastic forces placed upon them, tendons must be strong and rigid, yet flexible enough to participate in joint motion. Tenocytes, the regulatory cells inside the tendon, synthesize all of the components in the extra cellular matrix, including collagen. Collagen gives the tendon’s tough yet elastic structure, through packages of molecules formed into concentric fibrous bands.
Healing in healthy tendons is divided into three stages:
1. The first response after strain is inflammation, which supplies clotting to ruptured vessels inside the fascia, and absorbs the tissue that’s no longer viable.
2. At the proliferative and repair stage that follows, fibroblasts and tenocytes rush to the wound site, multiply, and also reconstruct the structure of the tendon.
3. The remodelling phase begins one to two months after injury, once the collagen fibres align in the direction of stress across the tendon. Through this procedure, tendons adapt and grow in thickness and length.
Historically, symptomatic tendons which failed to heal were assumed stuck in a cycle of inflammation and also the illness had been labelled tendonitis. Subsequent research has found evidence of degeneration in symptomatic tendons, and the inflammatory theory was then lost in favor of the expression ‘tendonosis’. More recent work suggests that both degeneration and inflammation exist in failed gut healing, called tendonopathy.
Tendonopathy
When excess loads, intrinsic or extrinsic variables, inhibit the usual healing response, the tendon becomes symptomatic (see box 1). Researchers at Melbourne have called this phase ‘reactive tendinopathy’, and explain the proliferation of collagen within the tendon as ‘non-inflammatory and short- term"(2). If the strain on the tendon remains, the fascia farther attempts to adapt by increasing the protein molecules in the extra cellular matrix and sprouting new blood vessels at the tendon, termed fig disrepair. Continued strain leads to tendon degeneration. However, if the load is modified before the tendon reaches the degenerative stage, the tendon may have the ability to recover through a normal healing response (see figure 1).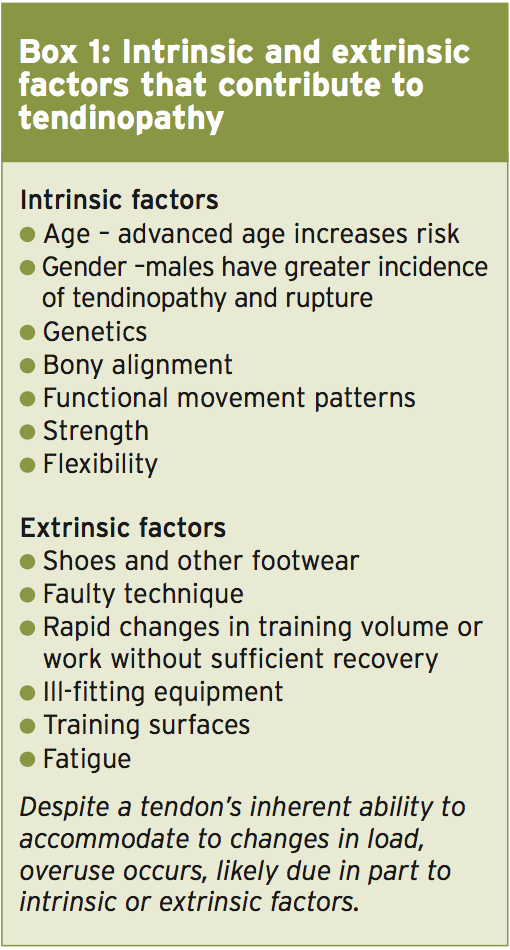
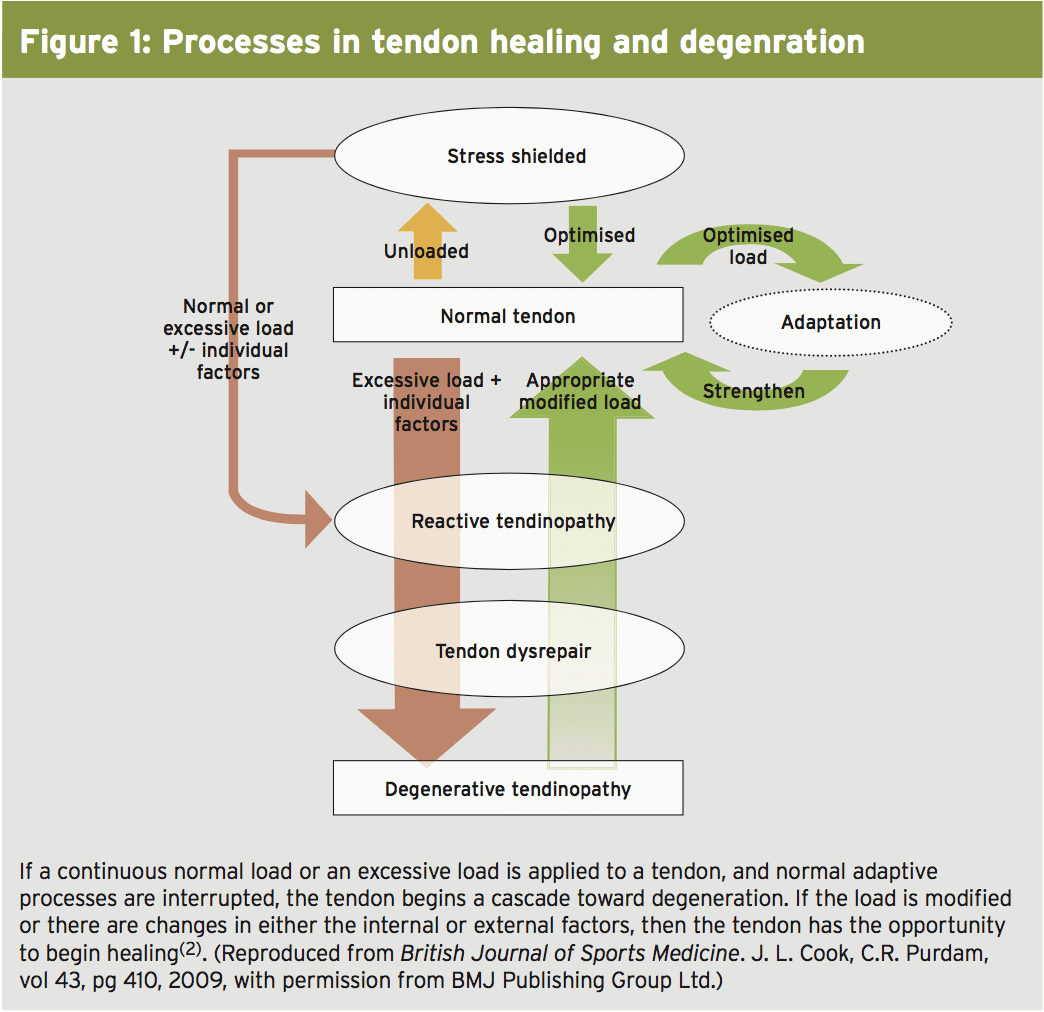
If a continuous normal load or an excessive load is applied to a tendon, and also normal adaptive processes are disrupted, the tendon begins a cascade toward degeneration. If the load is altered or there are changes in either the external or internal factors, then the limb gets the chance to start healing(two).
Anti-Inflammatory Interventions
Considering that the inflammatory part of Tendon recovery occurs after the initial strain, it’s sensible to think about anti- inflammatory drugs in treating tendonopathy, particularly in the period soon after trauma. Corticosteroid injections provide short-term pain relief from pain and swelling. Some assume that the result is actually about the cells surrounding the injured tendon, rather than the tendon itself(3). Knowing that corticosteroid injections are not curative but it’s important when considering their use in treatment. While enhancing comfort and operate in the short term, corticosteroids tend to weaken the construction of the tendon, ironically raising the risk of tendon rupture.Nonsteroidal anti-inflammatory drugs (NSAIDs), administered either orally or trans-dermally also assist with pain management. Professor Jill Cook has regularly stated that using Ibuprofen (and only Ibuprofen — maybe not Celebrex or Feldene etc.) appears to drop the pain in painful joints at the reactive phase if used short term(4). Again, some theorise that maybe the mechanism of activity is actually about the tissue surrounding the tendon. However, NSAIDs have been shown to supress tendon healing in animal research, which would indicate an immediate action upon the tendon(3). Since inflammation is a standard part of this adaptive answer, maybe inhibiting it with NSAIDs interrupts a necessary part of the recovery process.
The prolonged use of NSAIDs conveys a Risk of unwanted effects linked to the renal, cardiovascular and gastrointestinal systems along with a review of the literature provides little to substantiate their use in the treatment of tendinopathy beyond short-term pain control(3). Thus, the decision to recommend NSAIDs or not is based on clinical decision making. Consider the demand for pain management versus the potential side effects and impact on tendon healing prior to telling its use.
Healing Through Loading
Eccentric exercise is the most effective form of exercise for curing tendonopathy, although the mechanism of action is not well understood(5). During eccentric exercise (muscle lengthening), the tension within the muscle fibres is higher than when the muscles move concentrically (muscle shortening), yet the energy requirements, oxygen intake, adenosine triphosphate (ATP) breakdown, and heat generation are less than through concentric movement. Therefore, during eccentric exercise, the muscle produces exactly the exact same amount of work with less effort, and releases fewer annoying waste solutions.Maybe There’s something in this eccentric equation that allows the tendon to receive the mechanical stimulation it needs to repair, while keeping the bronchial Infection at bay. Employing the Melbourne model of degenerative tendonopathy, it’s sensible to expect a stressful load, along with the modification of intrinsic and extrinsic factors, to activate a normal adaptive response(two). Studies conducted on tendonopathic Achilles and patellar tendons show great results using an eccentric training program(3).
Strategies for treatment with eccentriclLoading typically rely on the Alfredson protocol. Alfredson and colleagues conducted a milestone Swedish research that showed heavy-load eccentric calf muscle exercise to be effective in treating chronic Achilles tendinopathy(6). Since then, most research suggest an identical regimen of three sets of 12-15 repetitions, first using body weight resistance and then progressing into a 15-repetition maximum immunity, twice daily(3). Pain is tolerated throughout the exercise; however, if significant pain persists following the workout, reduce the resistance.
Physiotherapy Modalities
Physiotherapists and trainers frequently strengthen Exercise prescription with different treatment modalities. Although these may increase the abstract relaxation of the athlete, they are not curative. For instance, cryotherapy (treating ice hockey) is a standard way of reducing inflammation and controlling pain. While powerful for acute harms, its efficacy in curing chronic tendonopathy from the disrepair phase is questionable.Question Of Blood Flow
Increased blood flow in damaged tendons, Nerves sprouting along side new blood vessels had been considered to be the cause of the pain in the rectal tendon. While some saw this increased vascularity since the body’s attempt to cure and sought ways to promote it, others concluded that preventing this angiogenesis would disrupt the failed recovery cascade and also provide pain relief.Shock Therapy
Theoretically, the administration of jolt Waves to an injured tendon causes micro trauma that stimulates blood flow. Extracorporeal shock wave treatment (ESWT) targets tissue using a single-impulse acoustic wave created using magnets, underwater electrodes, or crystals. Shock waves are uni-phasic and have a peak pressure that is nearly 1000 times larger than an ultrasound wave. Shock waves, treated as a low-energy therapy, need three weekly periods; where as, a high-energy treatment is one session which requires general or local anaesthesia.Writers from Queen Mary University of London lately reviewed the literature Limb tendonopathy and found just 13 Studies with enough reliable data to The protocol for government Of ESWT diverse between them, further Complicating the capability to draw definite conclusions. Nevertheless, the investigators Imply that ESWT is more effective in the Therapy of patellar tendonopathy than Other conservative treatments and equivalent to Patellar tendonopathy operation. When They also imply that ESWT is much more Effective than bizarre loading; and both Effective as eccentric loading when the tendonopathy is in the midportion of this Achilles tendon. There is some evidence That when combined, ESWT and eccentric Loading supply even greater outcomes(8).
Go With The Flow
There are many different treatments that aim to boost blood circulation to the relatively avascular tendon in an endeavor to boost healing. Topical glyceryltrinitrate, administered through a topical patch, delivers nitric acid (NO) to the tendon through the epidermis. The NO is supposed to improve collagen production and increase vascularization.Injections of platelet rich plasma, based on the subject’s own blood, directly into the tendon supposes that the platelets release growth factors into the tissue that is damaged (see Andrew Hamilton’s detailed article on platelet treatment elsewhere in this issue). These growth factors purportedly reduce inflammation and stimulate revascularisation and collagen production. Some have tried to inject whole autologous blood into diseased tendons with the very same targets.
All in all, the shortage of studies on the efficacy of each of the above mentioned treatments, as well as also the version in protocols, research design, and sample size make it hard to assess their effectiveness with complete confidence. In addition, some of those treatments carry with them significant risks or side effects. Professional licencing boards and government agencies vary on acceptance of those methods, including ESWT, to manage tendinopathy; clinicians should therefore carefully evaluate the pros and cons of a treatment choice before recommending its use for athletes.
Interrupting Blood Circulation
Though some treatments try to increase the blood flow to the damaged tendon others try to stop it. In sclerotherapy, a chemical agent injected into the tendon, causes thrombosis and corrosion of the newly formed vessels and nerves. Electrocoagulation utilizes a radiofrequency probe to transfer renewable energy into the diseased tendon and ruin the neovascular bundle. Injection with hypertonic glucose and lidocaine, called prolotherapy, works toward the exact same end whilst inducing an inflammatory response. The ability to test whether these remedies have the impact they intend is difficult. Studies showing their effect on pain and function are inconclusive(9,10).Researchers in Qatar, Italy, and England contested the validity of the theory of angiogenesis (new blood vessel development) as a source of either curing or pain in a joint evaluation of the literature about the subject(7). Conflicting evidence exists as to the presence of neovessels in symptomatic Achilles tendons.
The researchers reasoned that the presence or lack of neovessels bears no significance on the diagnosis, prognosis, or magnitude of pain experienced by people with tendinopathy. Consequently, the treatments that attempt to influence neovasculature one way or another, while originally promising, may end up being ineffective with nicely designed, randomised and controlled research. Until research provides better decisions, recommendation of those treatments to athletes isn’t worth the possible risks associated with them.
Surgical Options
Tendon surgery is generally considered a last resort for those who fail conservative therapy. Surgery removes the areas of diseased tendon, along with the accompanying neovascularisation, and arouses a fresh healing procedure. This is accomplished through ultrasound guided percutaneous tenotomy, occasionally called needling, or tendon debridement and repair via arthroscopic or open processes.Success rates following surgery vary, based on the type of procedure, the tendon medicated, and the amount of injury inside the tendon. Rehabilitation and return to sport can take upwards of 12 months, based again on the sort of procedure and severity of injury. Most notably, 20 percent to 30 percent of surgical treatments fail to increase the symptoms(10).
Future Treatments
Another potential treatment is the injection of cultured tenocyte-like cells, taken from the area’s own skin, into the injured tendon. These cells produce collagen and are thought to promote recovery. Preliminary studies show promise, but clinical trials are needed to confirm efficacy.Biomaterials, constructed from naturally occurring substances, have potential benefit in treating tendinopathy. All these biomaterials mimic native limb arrangement and therefore, drive cell production prior to alignment as normal tendon. In first stages of evaluation, this kind of tendon grafting has proved beneficial in canine areas(11).
Recommendations For Clinicians
Tendonopathy is among the most difficult sporting injuries to treat, and clinicians and athletes will grasp at almost anything with promise to stop the pain and return the player to game.Anti-inflammatory medications, used promptly following injury or the onset of symptoms, reduce pain but possibly deter healing. Physiotherapy modalities may subjectively assist with pain management but lack proof they’re curative. A number of different treatments, although theoretically sound, need more research and development, and proceed with them significant risks.
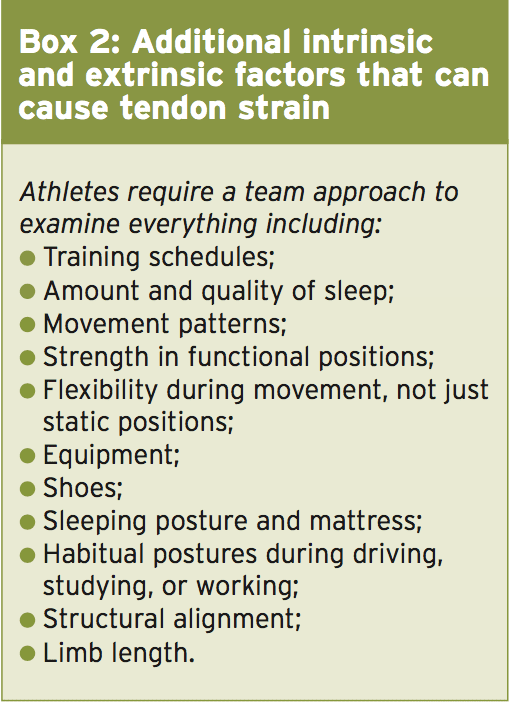
Modifying the load on the tendon through bizarre exercise and providing the tendon with adequate rest through the adjustment of contributing intrinsic or extrinsic factors, gives the tendon the very best opportunity to heal itself when in the reactive and disrepair phases (see Box 2). The tendon may endure the load for a weak link in the chain; be overworked since beginning twice-a-day practices; or be strained from unnatural placement while sleeping (as the athlete’s puppy insists on sleeping on the bed with its mind over the athlete’s knee. Play detective until you find and remove the cause of strain. Only then will the tendon get the rest it needs and begin to heal.
References
1.Birth Defects Res C Embryo Today. 2013 Sept;99(3):203-22
2.Br J Sports Med. 2009;43:409-16
3.Clin Sports Med. 2015;34:363-74
4. http://physioedge.com.au/wp-content/uploads/2011/10/Podcast-5-Jill-Cook.pdf
5. Int J Sports Phys Ther. 2011 Mar;6(1):27-44.
6.Am J Sports Med. 1998 May-Jun;26(3):360-6
7.Knee Surg Sports Traumatol Arthrosc. 2012 Oct;20(10):1891-4
8.Am J Sports Med. 2015 Mar;43(3):752-61
9.Clin Orthop Surg. 2015 Mar;7(1):1-7
10.Prim Care. 2013 Jun;40(2):453-73.
11.Adv Drug Deliv Rev. 2014 Nov 21. [Epub ahead of print]
