




Chiropractor, Dr. Alexander Jimenez explores the biomechanics of the popliteus muscle and considers its assessment along with effective rehabilitation.
Posterior knee pain is frequently associated with a number of structures comprising this area of the knee. The popliteus is a small muscle residing across the posterior aspect of the knee joint, in close proximity to an array of neurovascular structures. Due to its location and muscle action, the popliteus is a big player in the healthy functioning of the knee joint.
Injury to the popliteus muscle may arise in a weight-bearing position with a varus force to the knee whilst the tibia is externally rotated, or a forced hyperextension moment with the tibia internally rotated(1). During typical sporting movements such as football or netball – where the foot is planted by means of rubber soled or a studded shoe – the femur is forced to rotate externally on the tibia(1). It is uncommon that the popliteus is injured in isolation, and is usually accompanied by further injury to the posterolateral corner (PLC) or other surrounding structures(2).
Anatomy & Biomechanics
The popliteus muscle is a broad thin triangular muscle, which spans the majority of the space of the popliteal fossa at the back of the knee (see Figure 1A). Its origin is at the lateral femoral condyle of the femur and the lateral meniscus, and it then courses down and across the back of the knee joint to insert on the posteromedial aspect of the tibia(2). The popliteus tendon is positioned outside of the knee joint and the synovial joint lining, but does lie within the joint capsule as it passes through the popliteal hiatus (Figure 1B)(2). The popliteus is innervated from the tibial nerve roots L4, l5, S1(2).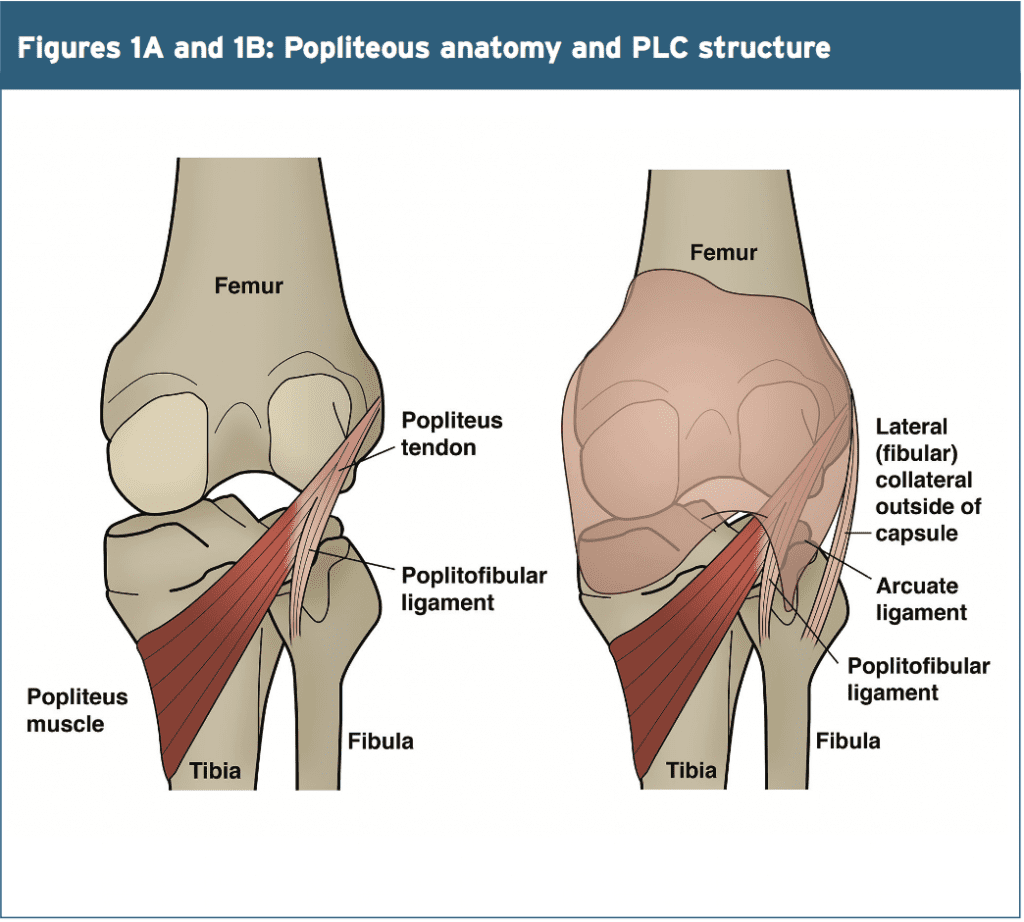
The popliteus is the primary internal rotator of the knee while in a non-weight bearing position. In contrast, popliteus externally rotates the femur on the tibia during load bearing which is often described as ‘unlocking’ of the knee joint. The popliteus therefore functions to provide both static and dynamic stability to the PLC of the knee joint. The PLC is a poorly understood area of the knee joint that can vary slightly from person to person; some authors have described no attachment of the popliteus to the lateral meniscus in 45% of cadavers(3). The PLC has also been referred to as the arcuate complex, comprising the fibular collateral ligament (also called the lateral collateral ligament, LCL), arcuate ligament, popliteus muscle and tendon, popliteal fibular ligament, fabello-fibular ligament and posterolateral capsule – see table 1 for more detail(2).

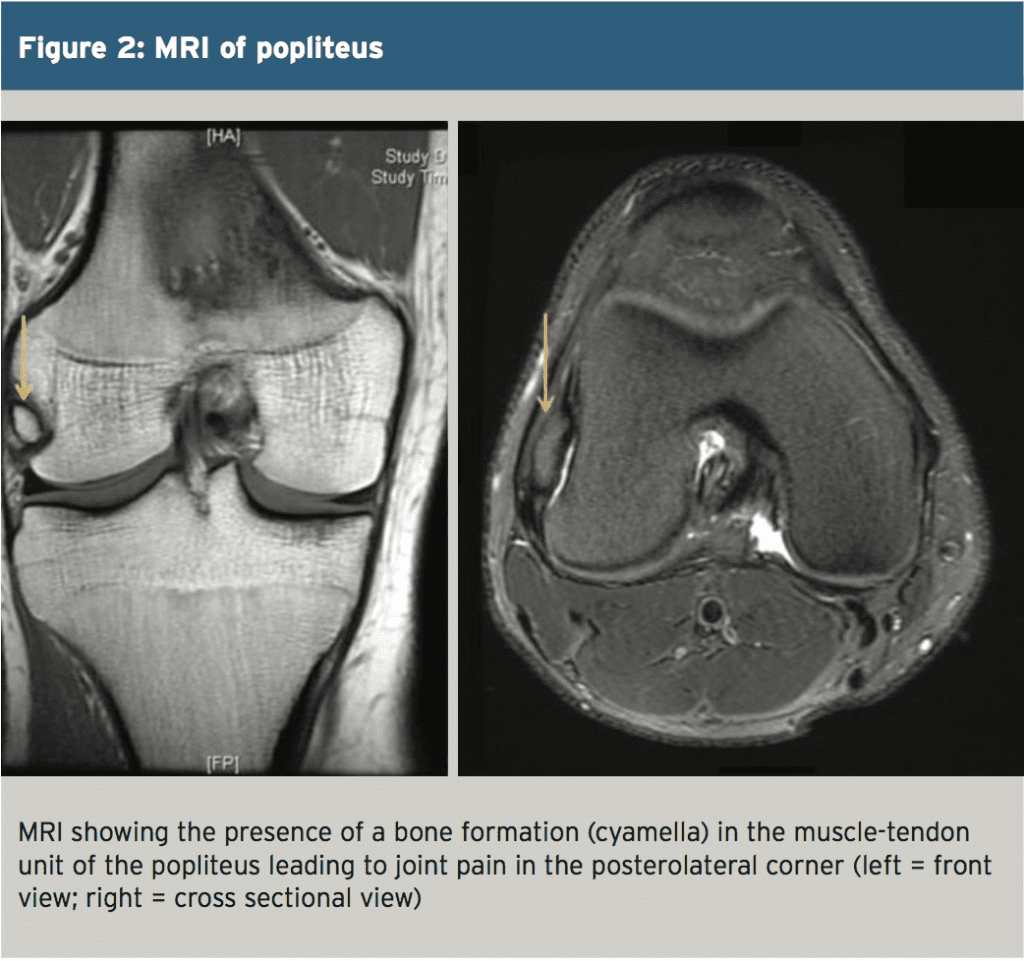
A 44-year old female complained of pain at the back and inside aspect of the knee after a stretching session. The patient presented with pain on weight bearing and found it difficult to walk on a flat surface and on stairs. An MRI (magnetic resonance imaging) scan indicated a cyamella in the popliteus and a low grade injury to the posterolateral joint capsule (see Figure 2). The cyamella was treated conservatively with the use of a knee splint, pain relief medication and the avoidance of excessive load bearing(5).
Despite this, clinicians should not assume that posterolateral pain at the knee joint is the result of a cyamella (and therefore just treat conservatively). Instead, it is recommended that an MRI scan is performed, especially if the patient is unable to weight bear pain free. The posterolateral corner of the knee in humans is essential for stability in an upright standing posture – far more than in many other animals such as cats and rabbits. In these animals, the occurrence of a cyamella is 100%, which is thought to be due to the flexed posture of the knee joint on loading(5). Therefore, any posterolateral pain in your patients should be examined with great detail.
Examination ascertained joint effusion and pain at the extreme ranges of movement. Tenderness was evident on the posterolateral joint line but there was no mediolateral or rotation instability. The motor function of the flexor hallucis longus (FHL), tibialis posterior (TP) and flexor digitorum longus (FDL) was recorded as nil but the patient had normal motor function of the gastrocnemius and soleus. Sensation was reduced in the plantar aspect of the foot but there were normal compartmental pressures in the lower leg (similarto that of the uninvolved limb).
A venogram was performed, which showed an obstruction of the deep venous system at the knee level, indicating compression of the surrounding extrinsic structures. An MRI showed that the popliteus muscle had ruptured with a hematoma in the upper calf fibres, causing pressure against the neurovascular bundle.
Six weeks of conservative treatment provided a decrease in pain, but no neurological improvement.
Electromyography indicated decreased nerve input activity of the FHL, TP and DFL muscles and decreased motor activity of the posterior tibial nerve. After 12 weeks the patient had developed paraesthesia to the medial calf and the medial plantar aspect of the foot. Repeated electromyography indicated no increased nerve activity. After 18 weeks the patient was able to flex his toes and invert his plantar flexed heel. Electromyography indicated increased nerve activity of the TP and the FDL. After 24 weeks the patient had regained normal function of the FHL.

A slightly different exercise performed in a load bearing position (Figure 4) uses a step of approximately 5-15cm, which is skid proof(1). The position of the stance leg on the step should be approximately 20-40 degrees knee flexion as a series of stepping tasks are carried out. Figure 4 outlines the different processes the leg steps into:
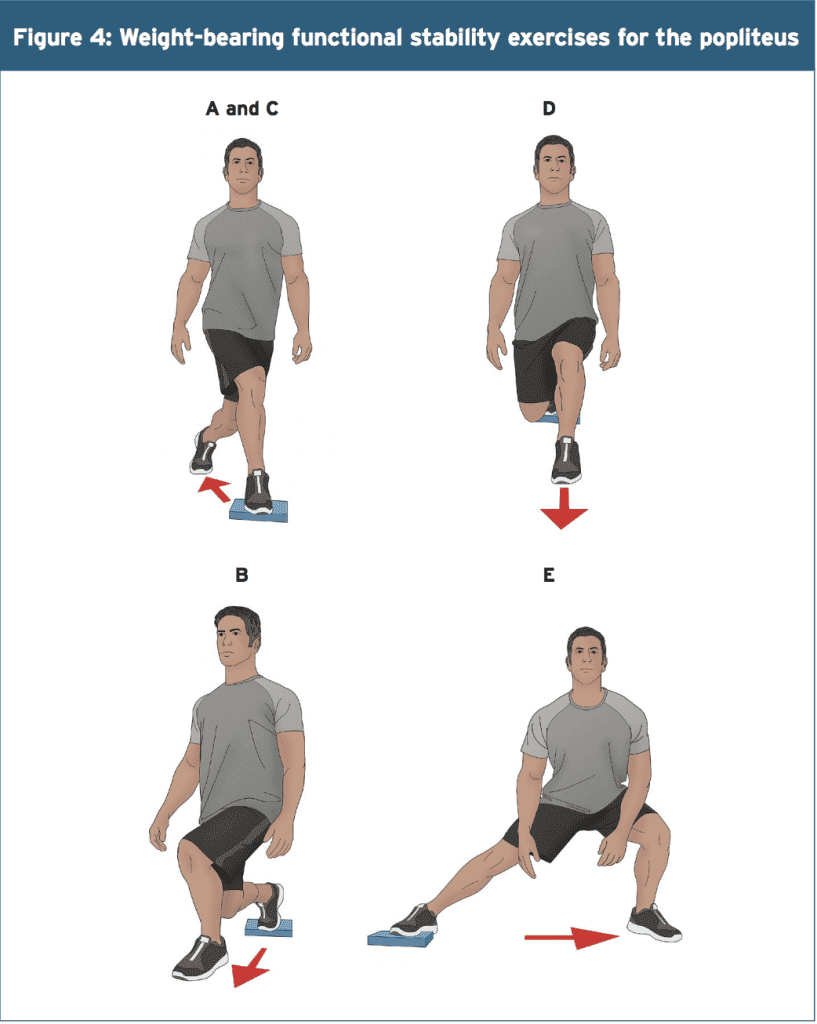
A) With the leg off the step
B) Stepping forwards and off the step into a crossover position
C) Returning to the starting position as in picture A
D) Stepping straight forwards as in a forward lunge
E) A side lunge out to the side
Throughout this process the same leg stays on the step and then it should be swapped over to repeat on the opposite leg. Nyland & colleagues stated that the stance leg of the exercise replicates some of the athletic demands produced during the mid-stance phase of different movements. In addition, the off-step movements replicate the initial and terminal swing phase movements, again replicating certain athletic demands. This exercise improves knee and hip stability in a functional manner.
The popliteus is reported as being rarely injured by itself and is likely to associated with other structures in the posterolateral compartment of the knee joint. The popliteus should be considered as injured if an acute heamarthrosis presents but without an indication of joint instability especially after a forced external rotation injury. Forced external rotation, with the foot planted and with the knee in slight flexion, is a key position for biomechanical loading of the popliteus.
References
1. J Orthop Sports Phys Ther, 2005, March, 35, 3
2. RG, 2014, 34, 2, 496 – 514
3. J of Bone and Joint Surg Am, 1989, 71, 5, 714 – 716
4. Curr Rev Musculoskelet Med, 2010, 3, 3–10
5. Radiology Case reports, 2014, 9, 1, 1 – 3
6. J Bone & Joint Surg, 1992, 74-B, 811-813
Posterior Knee Joint Assessment
It’s not possible to cover the entire assessment of the posterior knee joint in this article, but one review draws on the essential key elements that should be included. Clinicians from the University of California outlined the physical assessment of the posterior knee joint(4). They concluded that an assessment must include joint movements, muscle activity and ligament integrity testing. Instability of the PLC may involve a lesion to the popliteus but may also include some of the other structures of the PLC. Their recommendations are shown in box 1.Case Study 1
A case study published in 2014, by two radiologists in the USA, reported the case of a bone formation in the popliteus known as a sesamoid bone (same type of bone as a knee cap)(5). This sesamoid bone was referred to as a cyamella, and is a rare occurrence in the posterolateral corner of the knee at the point where the muscle and tendon of the popliteus is found.A 44-year old female complained of pain at the back and inside aspect of the knee after a stretching session. The patient presented with pain on weight bearing and found it difficult to walk on a flat surface and on stairs. An MRI (magnetic resonance imaging) scan indicated a cyamella in the popliteus and a low grade injury to the posterolateral joint capsule (see Figure 2). The cyamella was treated conservatively with the use of a knee splint, pain relief medication and the avoidance of excessive load bearing(5).
Despite this, clinicians should not assume that posterolateral pain at the knee joint is the result of a cyamella (and therefore just treat conservatively). Instead, it is recommended that an MRI scan is performed, especially if the patient is unable to weight bear pain free. The posterolateral corner of the knee in humans is essential for stability in an upright standing posture – far more than in many other animals such as cats and rabbits. In these animals, the occurrence of a cyamella is 100%, which is thought to be due to the flexed posture of the knee joint on loading(5). Therefore, any posterolateral pain in your patients should be examined with great detail.
Case Study 2
A further case study published in 1992, describes the mechanism and clinical presentation of a rupture to the popliteus in a 59-year old former professional American footballer(6). Severe pain and swelling presented two days following an external rotation twisting injury that was described as being in slight knee flexion with the foot planted.Examination ascertained joint effusion and pain at the extreme ranges of movement. Tenderness was evident on the posterolateral joint line but there was no mediolateral or rotation instability. The motor function of the flexor hallucis longus (FHL), tibialis posterior (TP) and flexor digitorum longus (FDL) was recorded as nil but the patient had normal motor function of the gastrocnemius and soleus. Sensation was reduced in the plantar aspect of the foot but there were normal compartmental pressures in the lower leg (similarto that of the uninvolved limb).
A venogram was performed, which showed an obstruction of the deep venous system at the knee level, indicating compression of the surrounding extrinsic structures. An MRI showed that the popliteus muscle had ruptured with a hematoma in the upper calf fibres, causing pressure against the neurovascular bundle.
Six weeks of conservative treatment provided a decrease in pain, but no neurological improvement.
Electromyography indicated decreased nerve input activity of the FHL, TP and DFL muscles and decreased motor activity of the posterior tibial nerve. After 12 weeks the patient had developed paraesthesia to the medial calf and the medial plantar aspect of the foot. Repeated electromyography indicated no increased nerve activity. After 18 weeks the patient was able to flex his toes and invert his plantar flexed heel. Electromyography indicated increased nerve activity of the TP and the FDL. After 24 weeks the patient had regained normal function of the FHL.
Rehabilitation
It is essential, during rehabilitation of an injured popliteus, to restore functional stability. Nyland and colleagues reported that improving gluteus medius and maximus activity can improve functional stability of the ankle and knee joints in the involved limb(1). The non-weight bearing exercise as depicted in Figure 3 promotes internal rotation of the tibia on the femur, and external rotation of the hip joint to promote gluteal activity. This exercise can be performed with or without a resistance band. It should be performed quickly on the concentric movement (but under control) but slowly on the eccentric phase, as the subject returns back to the starting position. Aim for 3-5 sets of 8-12 repetitions.A slightly different exercise performed in a load bearing position (Figure 4) uses a step of approximately 5-15cm, which is skid proof(1). The position of the stance leg on the step should be approximately 20-40 degrees knee flexion as a series of stepping tasks are carried out. Figure 4 outlines the different processes the leg steps into:
A) With the leg off the step
B) Stepping forwards and off the step into a crossover position
C) Returning to the starting position as in picture A
D) Stepping straight forwards as in a forward lunge
E) A side lunge out to the side
Throughout this process the same leg stays on the step and then it should be swapped over to repeat on the opposite leg. Nyland & colleagues stated that the stance leg of the exercise replicates some of the athletic demands produced during the mid-stance phase of different movements. In addition, the off-step movements replicate the initial and terminal swing phase movements, again replicating certain athletic demands. This exercise improves knee and hip stability in a functional manner.
Summary
The popliteus is an important active stabiliser of the knee joint and although it doesn’t maintain stability at the same level as the cruciate and collateral ligaments is importance is still of great magnitude. The popliteus should be assessed in detail using both weight bearing and non-weight bearing positions for assessment for dysfunction and instability in the knee joint.The popliteus is reported as being rarely injured by itself and is likely to associated with other structures in the posterolateral compartment of the knee joint. The popliteus should be considered as injured if an acute heamarthrosis presents but without an indication of joint instability especially after a forced external rotation injury. Forced external rotation, with the foot planted and with the knee in slight flexion, is a key position for biomechanical loading of the popliteus.
References
1. J Orthop Sports Phys Ther, 2005, March, 35, 3
2. RG, 2014, 34, 2, 496 – 514
3. J of Bone and Joint Surg Am, 1989, 71, 5, 714 – 716
4. Curr Rev Musculoskelet Med, 2010, 3, 3–10
5. Radiology Case reports, 2014, 9, 1, 1 – 3
6. J Bone & Joint Surg, 1992, 74-B, 811-813
