




Weak buttocks destroy the runner. Discover just how, by firming up your buttocks, you can improve your performance. Science based core chiropractor, Dr. Alexander Jimenez evaluates the case.
How many routine runners would suspect that the upper buttock muscle (gluteus medius) is the offender in very many running overuse injuries? This fact is less surprising once you understand that through running you're always either completely in the air or dynamically balanced on one leg -- and in both conditions the gluteus medius is a key muscle.
Situated on the upper edge of the hip (see below), gluteus medius is responsible for lifting the leg away from the body (abduction), enabling it to bend inwards and outwards, and crucially, keeping the pelvis stable in some certain situations, including the stance phase of running.
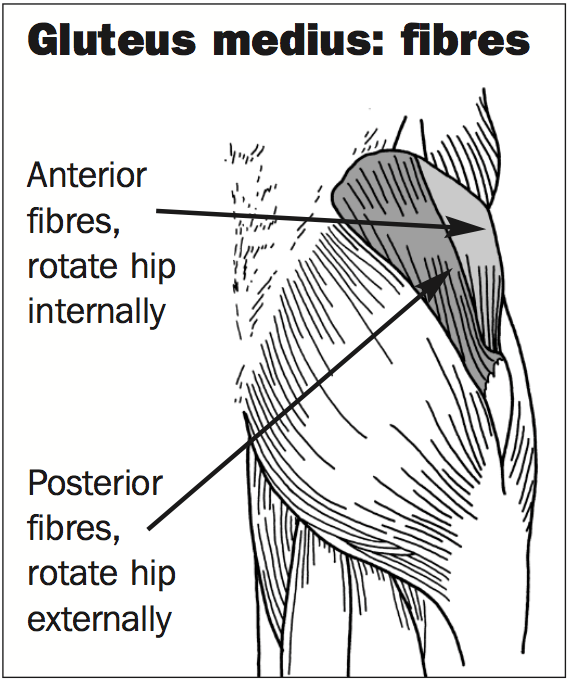
During right stance phase, for example, the muscle contracts to slow the downward movement of the left side of the pelvis so that the pelvis does not tilt heavily towards the ground. If the gluteus medius isn't working well enough to accomplish this control, the athlete is said to have a 'Trendelenburg gait'. Frequently, but not necessarily, the exact same weakness could be noticeable in walking, making a waddling motion or, in extreme cases, a limp.
Adaptations
Runners that have a weak or easily fatigued gluteus medius are very likely to make various adaptations to their technique, which can hide the true reason for a running injury. Table 1 lists the adaptations or cheating movements that happen through the stance phase of running.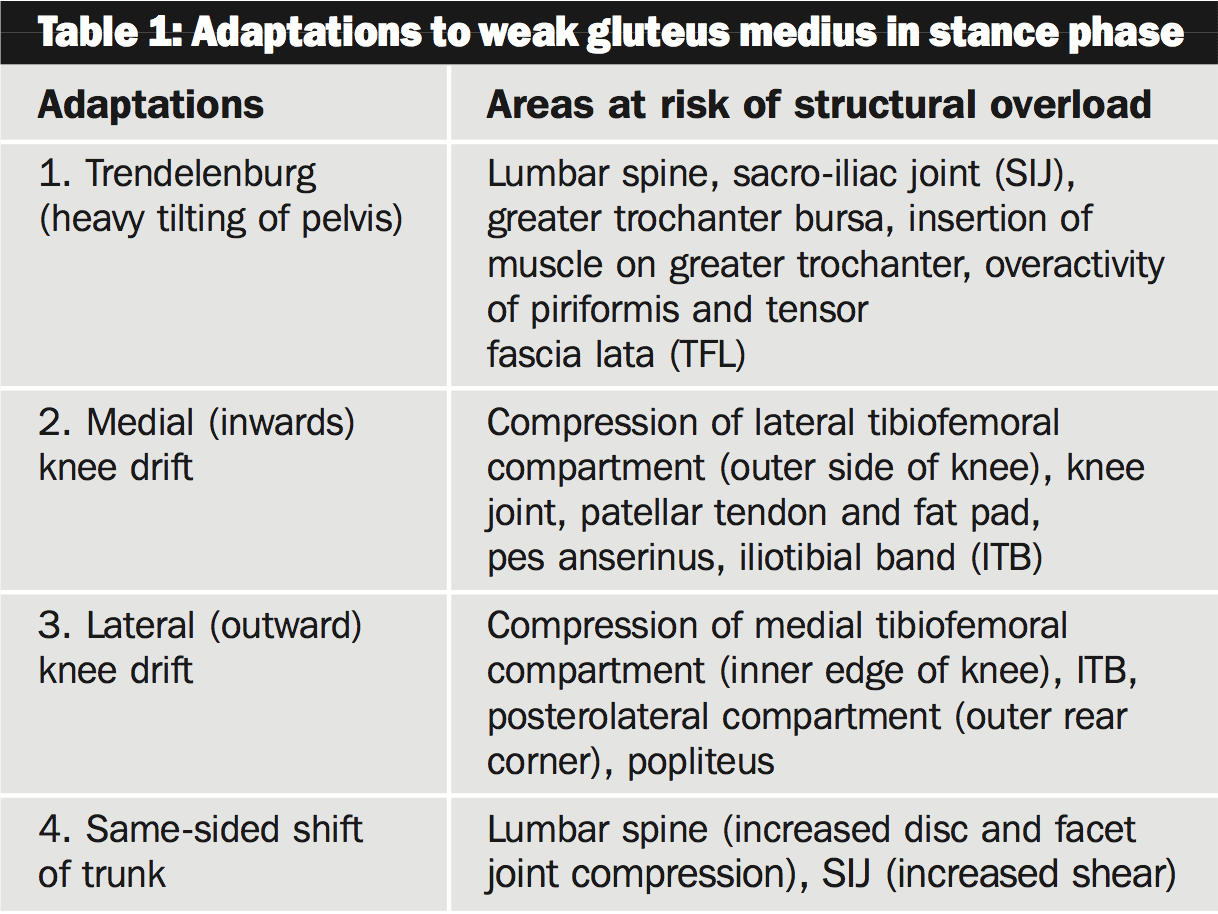
Adaptations 3 and 2 obviously cannot occur simultaneously, however a runner's technique may demonstrate a combination of adaptations, such as a mild Trendelenburg, inwards knee drift and a same-sided trunk shift.
In my experience, runners using inferior lively pelvic stability, for which gluteus medius is vital, will decrease their stride length and embrace a much more shuffling pattern to decrease the ground reaction force at contact and consequently the muscle control necessary to keep pelvic posture.
Weakness at gluteus medius will have consequences all the way down the kinetic chain. With Adaptation 2, for example, the buttock weakness will create inward drifting and rotating throughout the leg while running, which will leave the runner at higher risk of any condition concerning excessive or prolonged pronation of the foot, such as shin splints (medial tibial stress syndrome) or Achilles tendinitis.
An extremely informative analysis by Fredericson et al (2000)1 upholds the thought that gluteus medius weakness is a contributing element in ITB friction syndrome; affirms that injured and uninjured sides can be compared to ascertain weakness; also endorses retraining for strength gains as an effective treatment.
Fredericson measured hip abductor power in a group of injured male and female subjects, and found an average deficit of 2 percent in gluteus medius power on the injured side compared to the uninjured. Following a six-week retraining program, typical hip abductor torque improved by 34.9 percent for females and 51.4 per cent for males; 22 of the 24 injured athletes could return to running pain free. Above all, at a six-month follow-up no injury recurrences were reported.
Reference
1. Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC, Oestreicher N, Sahrmann SA, ‘Hip abductor weakness in distance runners with iliotibial band syndrome’. Clin J Sport Med. 2000 Jul;10(3):169-75.
The information contained in this publication is believed to be correct at the time of going to press. Whilst care has been taken to ensure that the information is accurate, the publisher can accept no responsibility for the consequences of actions based on the advice contained herein.
