




Swimming is renowned as a fantastic all-round sport with a low risk of injury -- but this doesn't equate to 'no' danger. Scientific chiropractor, Dr. Alexander Jimenez looks at what the current study has to say.
Swimming is a really low-impact sport where the loading is spread across a wide range of muscles and joints: hardly surprising, therefore, that it is often recommended since the low-injury threat sport for a vast range of participants. However, the low-impact nature of swimming does not signify that swimmers -- especially aggressive swimmers -- are immune from injury risk.
A glance at some numbers shows why: in a typical two-hour swimming session, an elite-level competitive swimmer could normally be anticipated to swim between 5,000 and 6,000 meters. This soon mounts up, with many competitive swimmers clocking up an average yearly mileage between between 20 and 40 kilometers -- that the aerobic equivalent of conducting 80 to 160 miles!
Broken down to limb movements, the figures are even more startling. On a typical training day, an elite swimmer can be expected to perform between 1,500 and 4,000 stroke cycles, which equates to anything up to 1,000,000 stroke cycles per training year(1,2). And because female swimmers, normally, have shorter arm strokes, they can execute an additional 660,000 stroke cycles per year -- ie over a 1.5 million annually(3)!
The causes of shoulder pain (that we'll look at in more detail later) are multifactorial but include the athlete's gender, their swimming experience, training space, stroke choice and workout intensity, the total amount of hand paddle use (that increases loading), and their upper-body strength and flexibility, and of course their prior trauma history(4,5).
Prevalence Of Shoulder Pain
Since then, other studies have looked into the incidence of shoulder pain among swimmers. A 1998 survey by McMaster and his colleagues looked at the correlation between shoulder laxity (see Box 1) and pain that interfered with instruction in a sample of competitive swimmers(7). It found that 35 percent of senior federal and Olympic swimmers experienced shoulder pain which prevented them from training efficiently. Other studies have variously noted that shoulder pain is the most frequent esophageal injury in swimmers, with a reported prevalence of between 40 percent and 91%(8-13).
This information was subsequently correlated with the amount of shoulder pain that the swimmers experienced and how much Feedback this caused them. Pain was rated in rest, with regular activities (eating, dressing, bathing etc), and with strenuous pursuits. The DASH sports module instructs participants to rate four objects (physical ability with sport technique, participation, satis- faction, and frequency), using a five-point scale, with '1' indicating no difficulty along with '5' signaling unable to participate within the last week.
Furthermore, several of physical steps were taken, including:
- passive range of movement (PROM) of both shoulders using an inclinometer for shoulder flexion in neutral rotation with the participant lying supine
- shoulder flexion, with the elbow maximally flexed for long head triceps tightness
- shoulder flexion, with the humerus externally rotated, knees and hips flexed, and abdominal muscles actively contracted for latissimus dorsi tightness
- internal and external rotation, with the shoulder abducted to 90 degrees
- maximal isometric force production for internal and external shoulder rotation with the participant lying prone and the shoulder abducted to 90 degrees
- scapular motion patterns during shoulder flexion and abduction, where the researchers looked for winging or dysrhythmia (using the scapular dyskinesis test – SDT)
- core muscle endurance using the side bridge, the prone bridge and the closed kinetic chain upper extremity stability tests (see Figure 1)
- pectoralis minor length measured from rib 4 to the coracoids process in a normal standing position (pectoralis minor length at rest) and when under- going a stretch.
The predisposing variables towards pain were not the same across all age groups; symptomatic swimmers who were less than 12 decades old tended to have diminished shoulder versatility, feebleness of the middle trapezius and shoulder internal rotators and latissimus dorsi tightness. By comparison, symptomatic swimmers that were 12 years of age or older tended to have pectoralis minor stimulation and decreased core endurance.
Shoulder Pain Causes
As was mentioned earlier, the reason behind shoulder pain in swimmers is very often multifactorial and includes(17,18):- incorrect stroke biomechanics
- overuse and fatigue of muscles of the shoulder, scapula, and upper back
- glenohumeral laxity with subsequent shoulder instability.
even with near flawless stroke procedure, there's ample opportunity for a shoulder injury to develop.
Impingement, Fatigue & Laxity
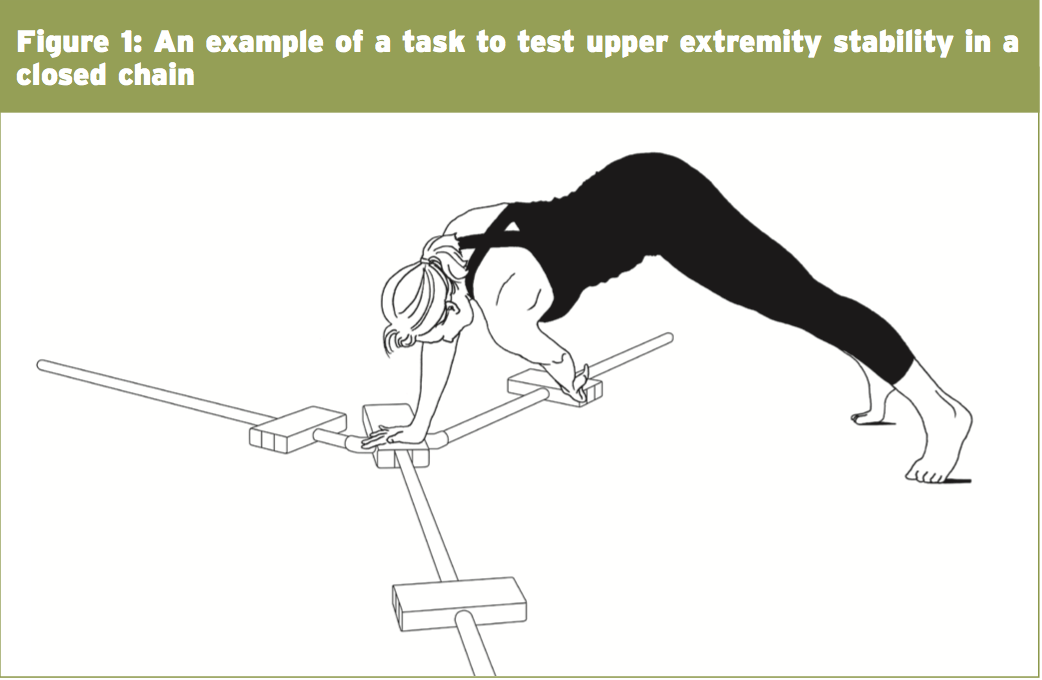
Impingement -- Shoulder impingement in competitive swimmers is usually brought on by altered kinematics because of muscle fatigue or laxity instead of pathological changes, which can be observed in other patient populations. Subacromial impingement can occur when the bursal surface of the rotator cuff impinges from the anteroinferior acromion.At the point when the hand enters the water, the hydrodynamic force applied on the hand by the water creates a massive moment in the shoulder joint, causing elevation of the humeral head and following impingement.
The hyperextension of the upper extremity in the late pull-through phase (submerged portion) of the stroke compels the humeral head anteriorly and moves it internally, which may aggravate an impingement when muscle fatigue is currently present.
Muscle fatigue -- Because the shoulder is an inherently unstable joint, adequate muscle strength is vital in order to maintain stability, appropriate stroke appropriate movement, and painless function. Much of the propulsive force in swimming is generated by adduction and internal rotation of the upper extremity due to pectoralis major and the latissimus dorsi muscles. Unfortunately, the training-induced adduction and internal rotation strength in swimmers can cause a strength imbalance, which leads to decreased glenohumeral stability.
The reason for this is that the teres minor muscle provides an external rotation pressure and stabilizes the humeral head in combination with the pectoralis major. The repeated contraction of those smaller stabilizing muscles during swimming makes them prone to exhaustion, increasing instability since they are less able to counteract the forces produced by the larger pectoral and latissimus muscles.
Laxity -- In most competitive swimmers, shoulder laxity with enhanced lateral movement of the humeral head could be seen(18). Although, there might be a hereditary element on the job in these swimmers, just around 20 percent of the subgroup meets the criteria for generalized ligamentous laxity(19). It's more probable the laxity increases over time as a result of continual overuse during competitive swimming. A certain level of glenohumeral laxity may be advantageous by allowing a swimmer to achieve both a body posture that reduces drag and a greater stroke length, both of which may help boost speed through the water. However, the diminished passive stability given by the glenohumeral ligaments in much more lax shoulders means that a greater contribution in the thoracic muscles is required to control the glenohumeral translation. This might cause muscle overload and subsequent muscle fatigue, with all the issues described previously.
Some common tests used to identify frequent shoulder pathologies in competitive swimmers are displayed in Table 1 below.
 Shoulder Pain Prevention
Shoulder Pain Prevention
As well as optimizing stroke biomechanics (see Box 2), a comprehensive program of stretching, strengthening, and endurance training ought to be considered as an essential part of each competitive swimmer's instruction program. Since musculoskeletal injuries in swimmers undergoing heavy training loads normally result from cumulative, repetitive injury, so it is critical that coaches and physicians carefully track each swimmer's training volume, intensity, and duration. This can help to minimize overuse injuries and identify people at risk.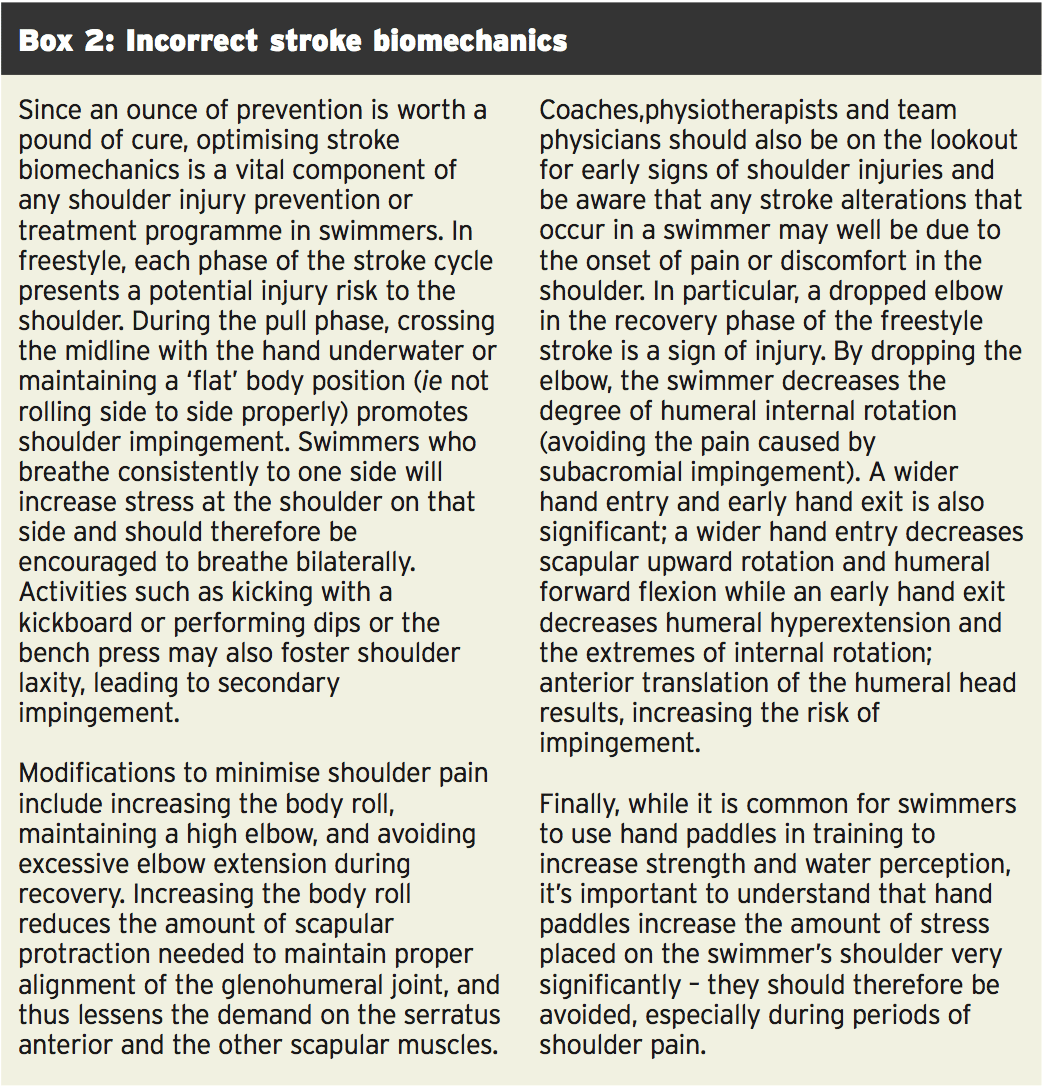
Meanwhile, scapular muscle strengthening can also be recommended to help improve glenohumeral stability. An endurance training and strengthening program for your shoulder and periscapular muscles, with emphasis placed on the serratus anterior, rhomboids, lower trapezius, and subscapularis, may assist in preventing injuries(17). Individual swimmers should be evaluated to determine endurance, strength, or flexibility shortages.
As soon as any swimmer experiences increased shoulder pain, their training program needs to be altered accordingly:
- Warm-ups should be extended with reduced intensity;
- The intensity, distance, and frequency of any subsequent training should be reduced;
- Painful strokes or positions (typically freestyle and butterfly) should be temporarily avoided (absolute rest is rarely indicated because it results in rapid de-conditioning of the elite swimmer);
- Hand paddles and pulling sets should be discontinued as they place stress on the shoulder and can exacerbate any injury;
- As an alternative, kick boards may be used with the elbows flexed to prevent shoulder impingement (this position may need to be modified to avoid forward shoulder elevation);
- Fins may also be used to maintain good body position while decreasing upper body stress;
- Pull buoys may also be useful as they can change the position of the shoulder in the water and reduce drag;
- Dry-land upper extremity weight training should be modified or eliminated;
- A strap placed around the upper arm over the biceps muscle (counterforce strap) may be useful to diminish the loading on the tendon.
Stretch Or Not?
Finally, it is worth mentioning extending. Most swimmers stretch but there is evidence that stretching may be more detrimental than useful(20). For example, the majority of the stretches which swimmers do stretch the lateral capsule of the shoulder. If the capsule is overstretched, the risk of uncertainty and subsequent injury increases, maybe permanently(19). Any extending, therefore, ought to be specific to the patient and designed to correct particular muscle or capsular tightness.Because swimmers generally have a relatively tight posterior capsule, which may encourage impingement pain, swimmers without pain should concentrate on extending the posterior capsule and anterior torso muscles. To selectively extend the posterior capsule without even stretching the scapular stabilizer muscles, it is necessary to stabilize the scapula. The easiest way to do so is to stretch the shoulder while lying supine, partially rolled onto the lateral border of the scapula.
In swimmers who've kyphotic posture due to tight anterior chest and shoulder musculature, stretching those muscles without stretching the anterior capsule helps reduce the forward shoulder posture and increase the subacromial area(5). Swimmers with shoulder pain ought to be instructed to stop all anterior capsule extending and rather focus on posterior capsule extending.
Swimmers with multidirectional instability or a background of subluxation should steer clear of all extending -- notably 'spouse extending' -- because it can easily force a shoulder beyond its normal limit and promote additional anatomic damage(19). For swimmers in whom extending is contraindicated, a gentle warm-up is sufficient to increase blood circulation to the muscles and get ready for the workout.
Summary
Correct stroke technique is crucial to help prevent harm and trainers should ensure that they carefully track training loads and identify stroke adjustments that may cause or change pain. Abdominal, core, scapular, and rotator cuff muscle strengthening exercises should be highlighted in a accident prevention program, and should the swimmer experience any shoulder pain, training intensity, distance, and frequency ought to be adjusted accordingly. Stretching is only recommended when a particular need has been identified.References
1. Am J Sports Med 1997;25(2):254-260
2. Clin Sports Med 1999;18(2):349-359
3. Scand J Med Sci Sports 1996;6(3):132-144
4. Clin Sports Med 2000;19(2):331-349
5. Sports Med 1996;22(5):337-347
6. Orthop Clin North Am 1977;8(3):583-591
7. Am J Sports Med 1998;26(1):83-86
8. Clin J Sport Med. 2010;20(5):386-390
9. Am J Sports Med. 1997;25(2):254-260
10. Scand J Med Sci Sports. 2007;17(4):373-377
11. Clin Sports Med. 1986;5(1):115-137
12. Br J Sports Med. 2010;44(2):105-113.
13. Int J Sports Med. 1995;16(8):557-562.
14. Stedman’s Concise Medical Dictionary for the Health Professions, ed 3. Baltimore, Williams & Wilkins, 1997, pp 446-446, 480
15. Arch Orthop Trauma Surg 2002;122(8):472-487
16. J Athletic Training 2012:47(2):149–158
17. Rodeo SA. Swimming. In: Krishnan SG, Hawkins RJ, Warren RF, eds. The Shoulder and the Overhead Athlete. Philadelphia, PA: Lippincott, Williams & WIlkins; 2004:350
18. Clin J Sport Med. 1996;6(1):40-47
19. Orthop Clin North Am. 2000;31(2):247-61
20. Physician and Sports medicine 2005; vol 33, no. 9
