




Balance and propioception training is commonly prescribed for the rehabilitation and avoidance of lateral ankle sprain injuries. But how effective is this strategy? Chirorpractor, Dr. Alexander Jimenez looks at recent evidence…
Ankle sprains are among the most common musculoskeletal injuries among sportsmen and women, and studies suggest that a significant proportion sports related injuries may be linked to ankle instability(1).
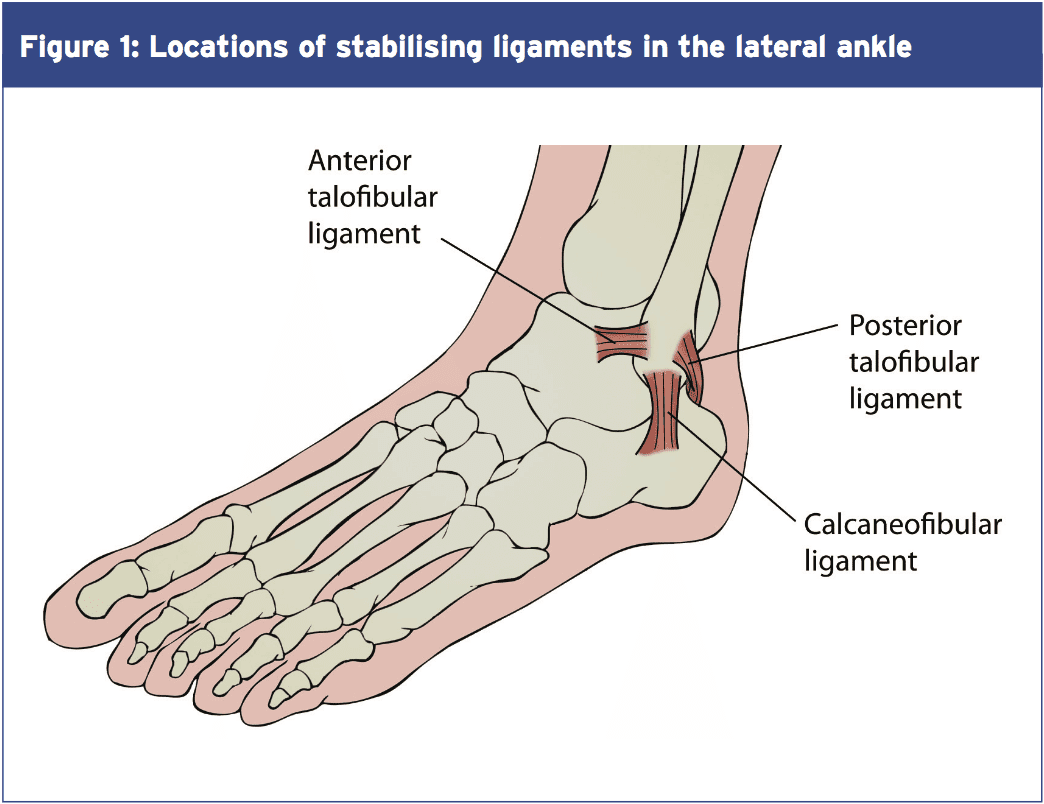
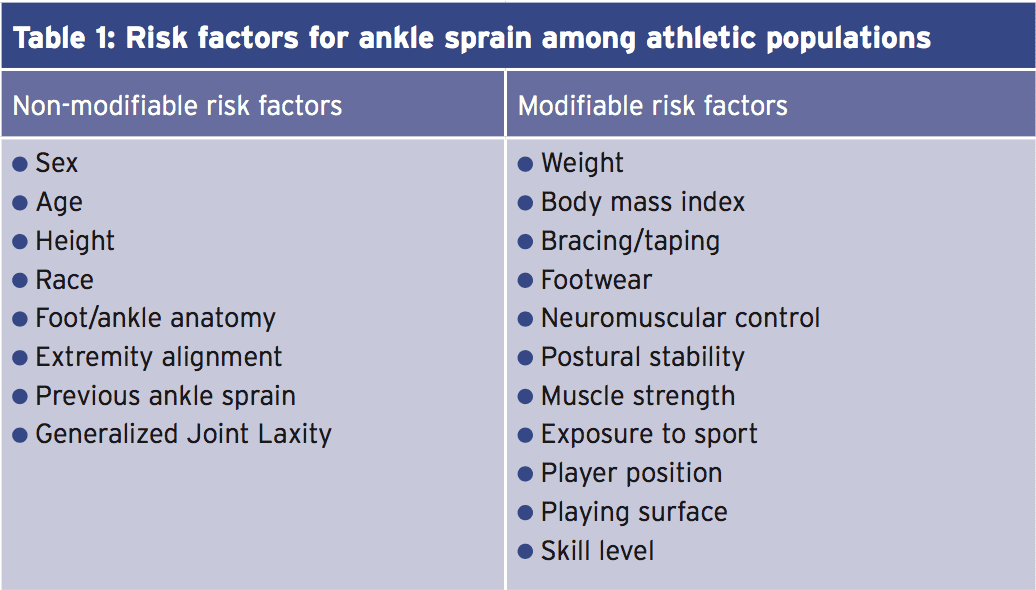
The most common single precipitating factor in lateral ankle sprain is really a single-limb landing on an uneven surface (2). In these circumstances, a quick and combined movement of ankle plantar flexion and inversion may lead to excessive lateral motion, resulting in ankle sprain. Another possible factor in determining the likelihood of lateral ankle sprain is proprioception, which is an important element of the neuromuscular control. With adequate proprioception, an athlete may have the ability to discover the speed and size of perturbation in a timely fashion, and react with appropriate muscle activation and joint movement. On the other hand, the nature of uneven terrain signifies that this is not always possible, even in athletes using exceptional propioceptive skills. Other elements having to do with the risk of ankle sprain in athletes have been shown in table 1 below.
That after an accident has occurred, re-injury is extremely likely. This is because injury/ harm to the lateral ligaments and joint capsule very often impairs the ability of the structures to offer optimum mechanical restraint following injury(3-10). Coupled with any deficits in propioception, this ends in a high re-injury rate. Indeed, studies have demonstrated that 73 percent of individuals who sprain their ankles are more very likely to undergo recurrent ankle injuries(11).
Balance & Propioception In Lateral Ankle Sprain & Re- Injury
But, despite decades of research on ankle sprain, the signs that this is the case remains inconclusive. Specifically, studies have failed to discover concrete proof that issues with ankle instability experience proprioception deficits in contrast to people with no history of ankle instability(12). This matter is further complicated by the fact that there is no standard testing and testing protocol for ankle proprioception.For many clinicians, the working assumption is that impaired proprioception and/or equilibrium play a significant role in the exposure to lateral ankle sprain. Additional lots of modern theory on this subject suggests that balance and coordination training may have both local and central effects on the sensorimotor system(15-19).
In an attempt to provide more clarity Seeing proprioception, balance and ankle sprain, a 2008 review analysis tried to answer the next three questions(20):
1. Can prophylactic equilibrium and coordination training decrease the risk of sustaining a lateral ankle sprain?
2. Can coordination and balance training Improve treatment outcomes related to severe ankle sprains?
3. Can balance and coordination training enhance treatment outcomes in patients with chronic ankle instability?
In total, the results of eleven research were united; three of which were used to answer Q1, three to reply Q2 and five to answer Q3. The researchers reasoned that prophylactic coordination and balance training considerably reduced the risk of ankle sprain in athletes, with the greatest effect observed in those with a history of sprain. There was also evidence that completing at least 6 weeks of coordination and balance training during recovery from a serious ankle sprain could substantially lower the risk of recurrent ankle sprain for up to 1 year.
However, the investigators also drew attention to how the advancements in instrumented measures of postural control associated with this training were not always measured from study to study, reducing the quality of the evidence. They also cautioned that the evidence was insufficient to evaluate the decrease in the probability of recurrent sprains, inconclusive to show improved instrumented postural control steps, and limited with respect to developments in self- reported role in athletes with chronic ankle instability who complete equilibrium and coordination training.
The findings from the preceding study match with a rather recent study into ankle sprains from the athletic people(12). This study acknowledges that modified neuromuscular control because of peripheral proprioception affects of the ankle joint may donate to the high recurrence rate of lateral ankle sprain, which after the first trauma, overstretched/loosened ligaments and joint capsule might hamper the function of those mechanoreceptors in those constructions. It also reports that some investigators have reported protracted peroneal muscle reflex latency in injured ankles(21,22), and ankle position sense deficits in several testing protocols(23-25).
However, the researchers go on to point out that despite this evidence, there are also numerous studies that contradict those findings. For instance, in studies comparing healthy and unstable ankles, no peroneal reflex latency differences (26-28), no place sense differences(29-31), and no movement sense gaps(32) were found between healthy and unstable ankles. In addition, a few studies indicate that the ability to sense ankle position isn’t a fantastic predictor for future ankle sprains(33).
Balance & Strength
One of the face of it, it seems as though the Evidence is conflicting — ie that balance training does appear to improve the prognosis for shoulder sprain and reduce re-injury rates, but that there’s little evidence that enhancing propioception/ neuromuscular control produces positive results. Maybe that since with better/intact proprioception at the ankle joint, generating sufficient muscle power that is fast enough to battle big and fast perturbations such as landing on an uneven surface is still a issue.One possible explanation for the Observations is the role of strength. A recent study has argued that improving muscle power might actually play a more important role in ankle sprain prevention and rehabilitation than enhancing proprioception(12).
Although larger muscle activation can However, what it might do is to help restore ankle muscle balance, place the ankle in more secure position (eg longer dorsiflexion using a stronger tibialis anterior) and increase the strength of ligaments. In addition, a larger/ stronger muscle may also provide extra passive restraints to the ankle joint.
It follows from the above therefore that If balance training is advantageous in reducing the episodes of ankle sprains, it is most likely due to enhanced stiffness and strength in both ligaments and muscles in the ankle joint rather than improved neuromuscular control. To put it differently, while enhancing cerebral control and proprioception in the ankle joint can be ineffective at protecting the ankle from large and fast perturbations, balance training can increase the strength of muscles and ligaments around the ankle joint. Since ligaments would be the principal stabilizer of the ankle joint, treatment protocols with a balance training element may benefit the subjects with unstable ankles.
Summary
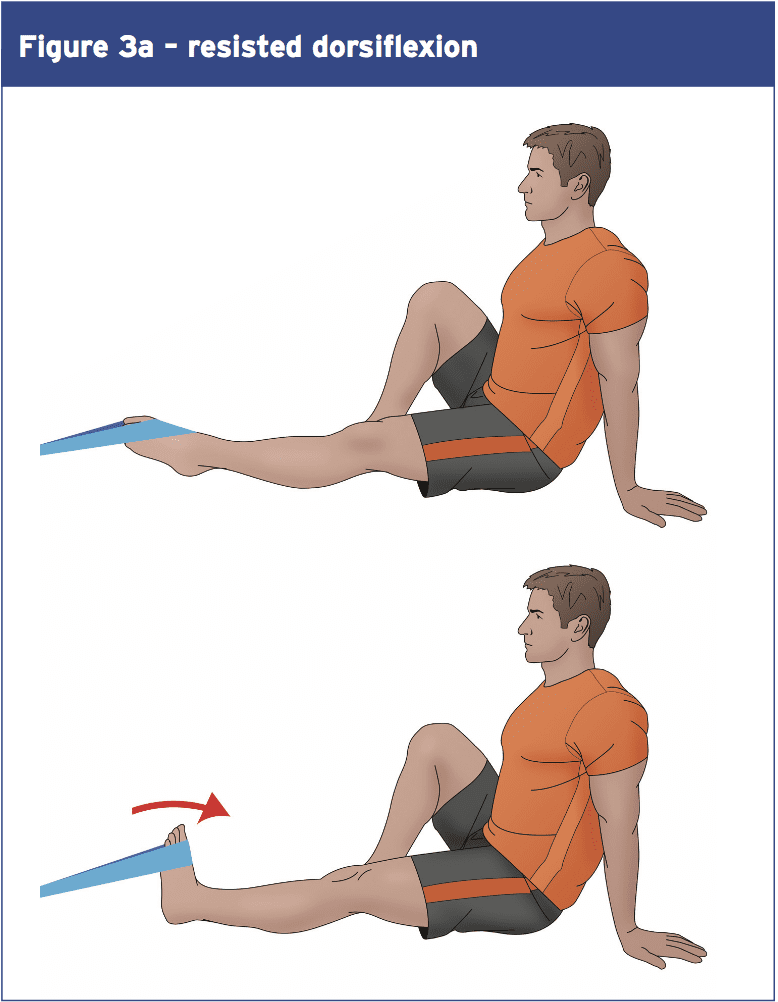
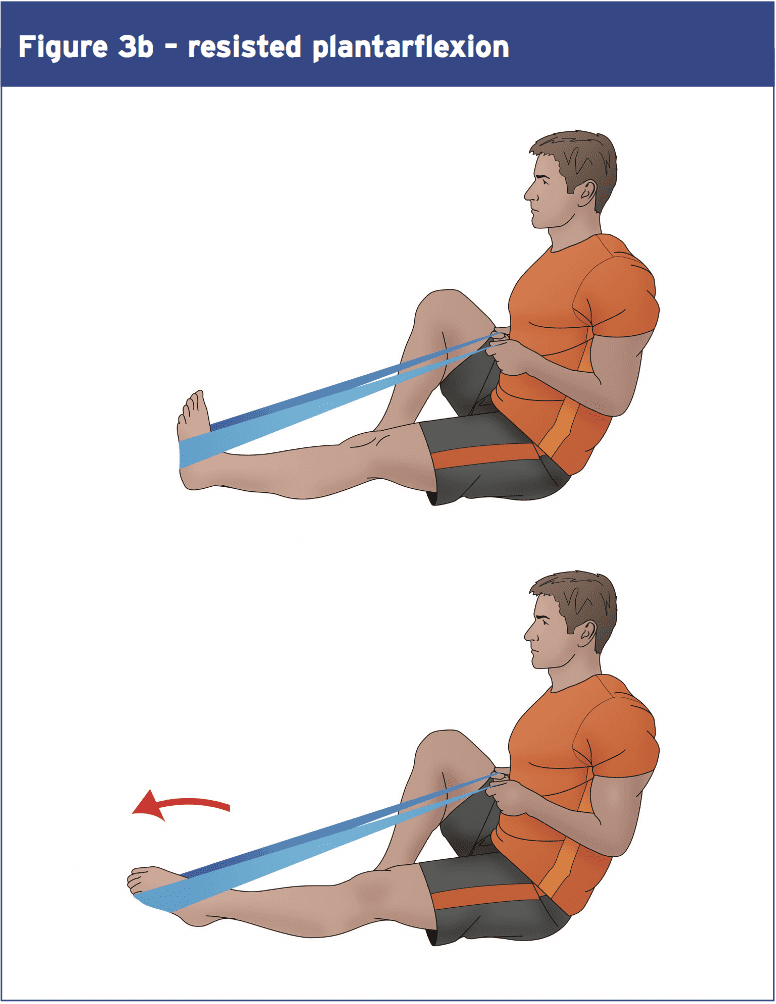
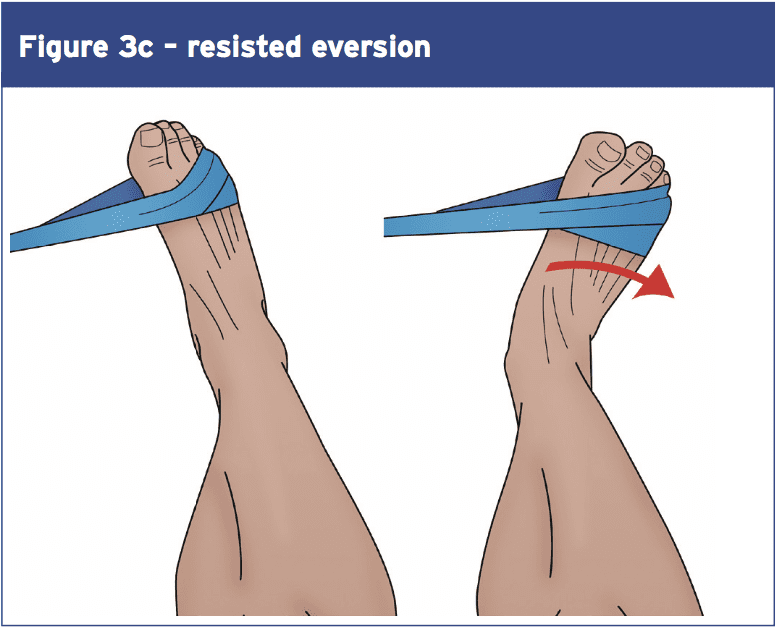
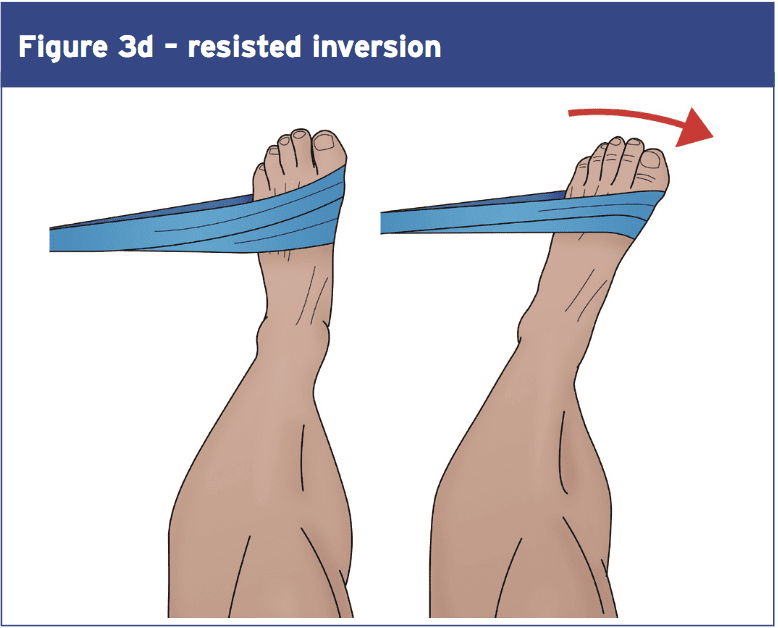
Looking at the overall signs, what can we conclude? Firstly it appears that ankle injury prevention and rehab programmes that concentrate purely on propioception improvement are most likely to be of limited value–theevidencethatpropioceptive training confers benefits in terms of first injury prevention or recurrence is rather weak. The evidence for equilibrium training however is much more powerful — although the benefits are likely to happen as a consequence of improvements in muscular and ligament strength.Although more study is needed in this place, the evidence so far suggests that improving ankle strength may be a V\valuable part of any prevention/rehab program. Studies reveal that Thera-Band or multi-axial ankle exercises Are successful in building ankle strength (for platarflexion and resisted ankle eversion and inversion – see Figures 3 a,b,c, and d). One study found increases of 20-50\% over a 6-week intervention application (37). Balance protocols on wobble boards can Also be adapted to help develop higher Levels of ankle strength — such as by Holding increasing quantities of weight Increasingly more elevated positions During equilibrium instruction. 1 study found gains of 20-50\% more than a 6-week intervention application (37). Also be accommodated to help build higher Levels of ankle strength — such as by Holding increasing amounts of weight at Progressively more elevated positions during balance training.
References
1.Conscious Cogn 2003; 12: 609-619
2. Foot Ankle 1990; 11: 41-44
3.Aust J Physiother 2007; 53: 193-198
4.J Athl Train 2012; 47: 444-456
5.J Athl Train 1997; 32: 221-225
6.J Athl Train 2002; 37:487-493
7.J Orthop Sports Phys Ther 2003; 33:166-173
8.J Orthop Sports Phys Ther 2013; 43: A1-40
9.Am J Sports Med 2005; 33: 1174-1182
10.J Bone Joint Surg Br 1965; 47: 678-685
11.Br J Sports Med 1994; 28: 112-116
12.World J Orthop 2015 June 18; 6(5): 434-438
13.J Athl Train. 2002;37(4):413–429
14.Clin Sports Med. 2004;23(1):83–95
15.J Athl Train. 2002;37(4):364–375
16.Sports Med. 2000;29(5):361–371
17.J Athl Train. 2002;37(4):386–393
18.Med Sci Sports Exerc. 2004;36(3):388–396
19.Am J Sports Med. 2003;31(4):498–506
20. J Athl Train 2008;43(3):305–31
21.Am J Sports Med 1995; 23: 414-417
22.Am J Sports Med 1992; 20: 257-261
23.J Sci Med Sport 2010; 13: 2-12
24.Clin Biomech (Bristol, Avon) 2008; 23: 1065-1072
25.Clin Biomech (Bristol, Avon) 2014; 29: 977-983
26.J Orthop Sports Phys Ther 1997; 26: 73-77
27.Clin Orthop Relat Res 2000; (375): 193-201
28. J Athl Train 2002; 37: 475-480
29.Scand J Med Sci Sports 1999; 9: 104-109
30. Phys Ther 1987; 67:1505-1509
31.Br J Sports Med 2011; 45:660-672
32.Aust J Physiother 2007; 53: 193-198
33.Scand J Med Sci Sports 2005; 15: 336-345
34. J Bone Joint Surg Am 1955; 37-A: 1237-1243
35. Clin Orthop Relat Res 1972; 85: 50-58
36.Clin Biomech (Bristol, Avon) 2013; 28: 524-529
37. J Athl Train. 2012 May-Jun; 47(3): 282–288
38. Sports Health. 2012 Nov;4(6):504-9
39. Am J Sports Med. 2001;29(1):31-35
