




Chiropractor, Dr. Alexander Jimenez looks at the evidence for blood flow restriction training; does it benefit athletes who require rapid post-injury rehab and if so, how should it be performed.
Introduction
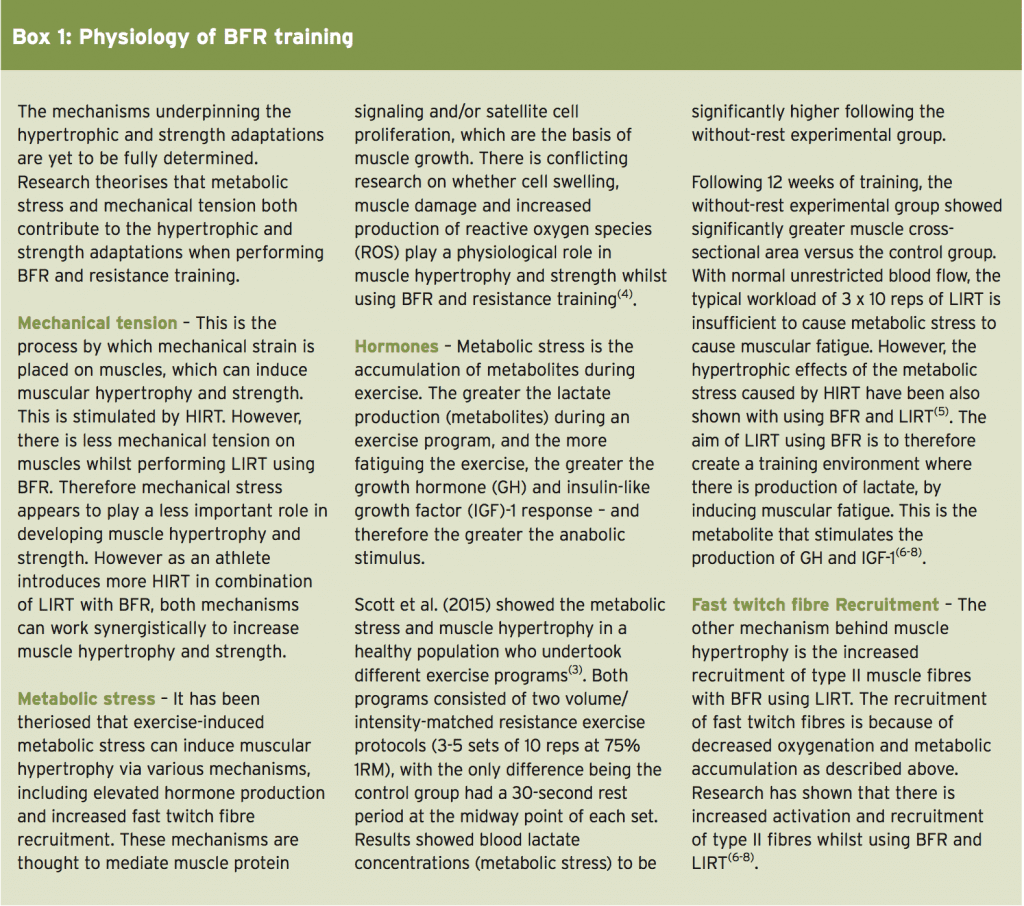
An inevitable consequence of lower limb injuries is muscle atrophy and weakness. Rehabilitation therapists and coaches want to find ways to limit this from happening, so an athlete’s recovery is speedy, safe and injury recurrence is prevented.A traditional method of training athletes to increase muscle size and strength is high intensity resistance training (HIRT) with multiple sets of 5-12 repetitions at loadings greater than 70% of a single repetition maximum (1RM)(1). However, following an injury or surgery, it may not be possible to perform HIRT. Indeed, it may even further damage healing tissue and therefore cannot be performed at all. By contrast, low intensity resistance training (LIRT) at reduced intensities (20-50% 1RM) in conjunction with blood flow restriction (BFR) has been shown in research to be effective at increasing muscular hypertrophy and strength(2).
What Is BFR Training?
BFR training is achieved by the use of inflatable pressurised cuffs or tourniquets around a limb (proximal to the muscle being trained), which limits blood delivery to and from the contracting muscles (see Figure 1). Currently there are no standardised recommendations for the applications of BFR during LIRT(3). However, it is important that an evidence- based, safe approach is used when applying BFR during resistance training. This article looks at the physiological mechanisms behind BFR with LIRT (see Box 1), and when and how it is currently used to rehabilitate athletes at the GWS Giants football club for lower limb injuries.
When Is BFR Training Used?
Following an injury or surgery, atrophy of surrounding muscles is very common. For example, following ACL reconstruction, quadriceps muscle wasting is evident within the first week post operatively. Prevention of muscle atrophy and increases in strength is associated with greater athlete performance. It is therefore vital to restore muscular hypertrophy and strength to allow for a safer and quick return to play for an injured athlete. During the acute phases of rehab, it’s important to protect the healing tissue. HIRT, a traditional training modality for increasing muscle hypertrophy and strength may be contraindicated as it may further injure or compromise healing of an injured structure. For example, following a reactive patellar tendinopathy, the tendon cannot withstand HIRT. If the athlete is subjected to heavy resistance training, the tendon may become more painful and even further injury can occur.There are only three studies that have utilized BFR in a rehabilitation based setting(9-11). Two of the studies are case studies only(10,11). One well-conducted study by Ohta et al examined a 16-week LIRT program using BFR on knee extensor and flexor strength following an ACL reconstruction(9). Results showed strength was better maintained pre/post operation and between injured/uninjured limbs for the BFR group. The BFR group also showed a trend towards a significant increase in cross-sectional area of the knee extensors with no change in the control group.
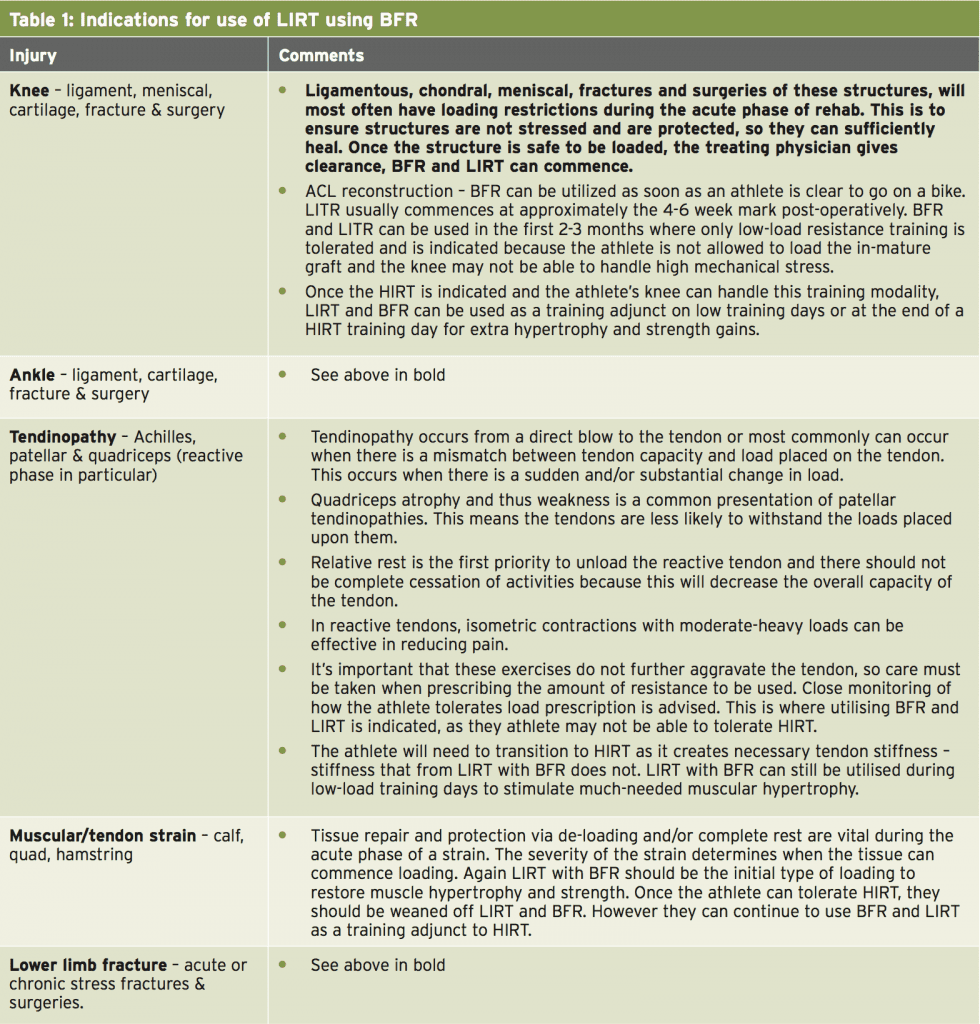
Although there are no other high quality studies that focus on rehabilitation, there is a lot of evidence that shows BFR and LIRT can increase muscular hypertrophy and strength. Clinically, athletes with specific injuries could benefit from this type of training to accelerate their rehabilitation and return to play. The rehabilitation coordinator must liaise with the team sports physician or surgeon to get clearance to use BFR on athletes. Injuries that can benefit from LIRT using BFR are any lower limb injury (see Table 1).
Methods Of BFR Training
There are a number of variables to consider when applying BFR and using LIRT. These include:- Type of cuff and occlusive pressure
- Training protocol
- Safety considerations
Type of cuff and occlusive pressure
Two important factors when using BFR are cuff width and cuff pressure. The cuff pressure in the literature is highly variable between studies. Moderate cuff pressures are recommended typically 1.3 times above systolic blood pressure (>120mmHg) or between resting diastolic blood pressure and systolic blood pressure (80-120mmHg)(2,7,12). Safe application using the Sports Rehabilitation Tourniquet (SRT), which is an inflatable cuff of pressures between 90-150mmHg (ideally > 120mmHg). See video below or use this link for correct application of the SRT: https:// www.youtube.com/watch?v=4J6KiXpl3sYOcclusion Cuff Training
Training protocol
A typical protocol used in the literature whilst performing BFR with LIRT is 1 set of 30 repetitions, followed by 3 sets of 15 repetitions with 30-60 seconds of rest at a load of 20-30% 1RM(12). It is important to note however that because of injury, an athlete may not be able to complete this amount of repetitions and sets, as it may induce too much mechanical stress. This may interfere with healing, re-aggravate an injury and even further injure the athlete.Once an athlete has been cleared to commence LIRT using BFR its important to progress with caution and the protocol may be as little as 3 sets of 10-12 repetitions with a load of 20% 1RM. As the athlete improves they will be able to tolerate more repetitions, sets and loading. Once an athlete transitions from LIRT to the desired HIRT, BFR training can be used as an accessory training modality. For example, after a lower body HIRT session, some LIRT accessory lifts for quadriceps hypertrophy can be used, such as single leg squats or knee extensions with BFR.
LITR using BFR can also be used on low-load training days, when a HIRT is the main focus of the athletes training regime. For example if an athlete is to complete HIRT 3 times per week, LIRT using BFR can be utilized on two other days (see Table 2). When utilizing LITR with BFR, its important to cause metabolic stress whilst training; therefore short rest periods are key. Sets do not have to be performed to muscular fatigue(7). Working to fatigue is a form of maximal training and may induce too much mechanical stress for the injury. The recommended training protocol for BFR and LIRT is shown in Table 3. The occlusion should remain on for the entirety of the sets for an exercise to allow for metabolites to accumulate.


Summary
LIRT at reduced intensities in conjunction with BFR has been shown in research to be effective at increasing muscular hypertrophy and strength. More research needs to be done using BFR and LIRT with the injured population. Through the mechanisms described above, BFR and LIRT is a helpful training tool that can be used for injured athletes in early stages of rehabilitation, and as an accessory to HIRT. HIRT must not be forgotten, as this traditional training modality is important in building muscular strength and hypertrophy, which is vital in the later stages of rehabilitation before return to play.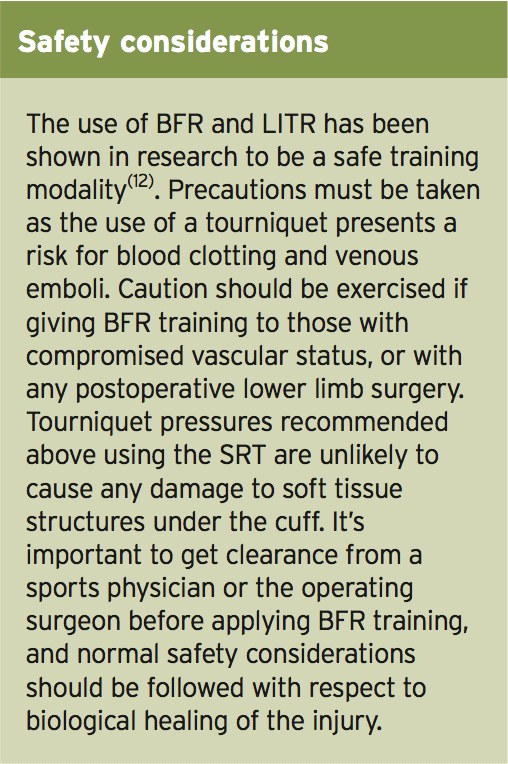
References
1. Med Sci Sports Exercise 2009, 41(3):687-708.
2. European Journal of Applied Physiology 2012. 112, 1849-1859.
3. Sports Med 2015. 45:313–325.
4. Med Sci Sports Exercise 2005, 37 (6), 955-963.
5. Medicine and Science in Sports and Exercise 2007, 39(10), 1708-1713.
6. Sports Med 2015, 45, 187-200
7. Acta Physiologica Hungarica 2012, 99(3), 235-250.
8. Journal of Australian Strength and Conditioning 2015, 23(4), 57-68.
9. Acta Orthopaedica Scandinavica 2009, 74(1), 62-68.
10. Journal Kaatsu Training Res 2005 1, 29-32.
11. Journal of Bodywork & Movement Therapies 2013. 17, 42-45.
12. Scandinavian Journal of Medicine & Science in Sports 2011. 21, 510-518
