




Sciatic Nerve Entrapment
- Piriformis Syndrome
- Peroneal Nerve Entrapment
- Tarsal Tunnel Syndrome
Sciatic N. Piriformis Syndrome
 Causes
Causes
- Anatomic variation
- Piriformis overuse/tension
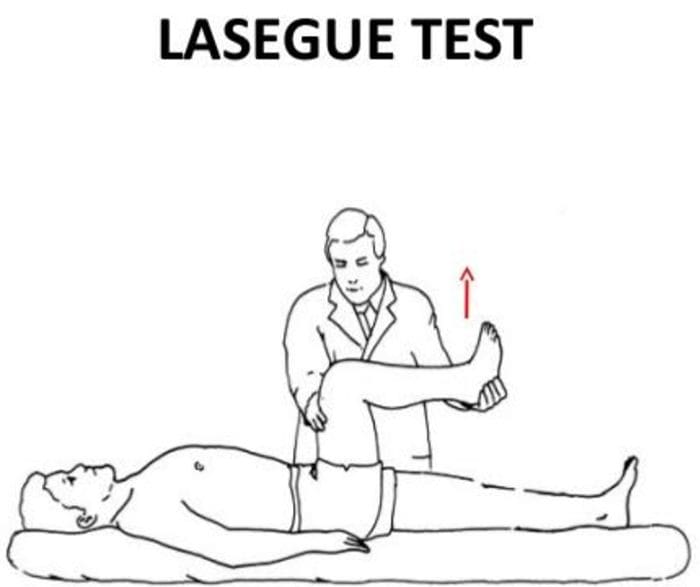
Exam
- Positive Lasègue test possible
- Doctor extends patient’s leg passively, while patient is lying supine positive test if maneuver is limited by pain
- Tenderness and palpable tension in piriformis muscle which elicits symptoms
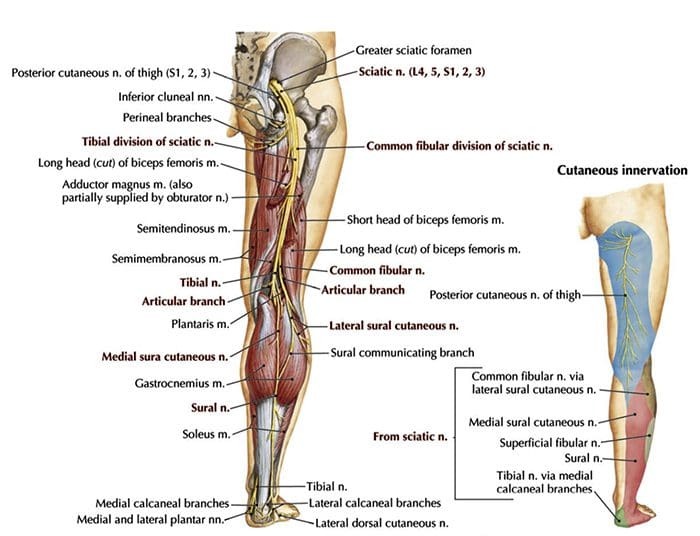
Sciatic N. Peroneal Nerve Entrapment
- Peroneal or Fibular branch of Sciatic nerve entrapped at the fibular head
- Tinel’s sign may be present at fibular head/neck
- Usually affects common peroneal nerve, therefore motor and sensory symptoms can be seen
- Weakness of ankle dorsiflexion and eversion (tibialis anterior m.)
- Sensory disruption on the dorsum of the foot and lateral aspect of the calf
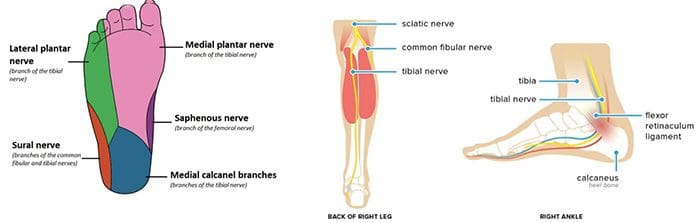
Sciatic N. Tarsal Tunnel Syndrome
- Tibial nerve impinged in the tarsal tunnel
- Sensory changes in the sole of the foot
- Tinel’s sign may be present with percussion posterior to the medial malleolus
Radiculopathy
- A mononeuropathy – located in one specific area
- Neuropathy involving spinal nerve roots
- Presents as changes in sensory and/or motor function affecting a single or a few nerve root level(s)
- Most commonly seen radiculopathies include:
- Sciatica
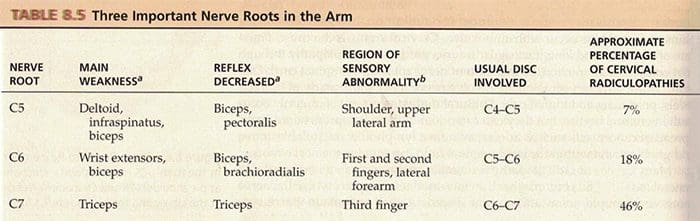
- Cervical radiculopathy
Common Causes Of Radiculopathy
- Disc herniation
- Osteophytes
- Spinal Stenosis
- Trauma
- Diabetes
- Epidural abscess or metastasis
- Nerve sheath tumors (schwannomas and neurofibromas)
- Guillain-Barré syndrome
- Herpes Zoster (shingles)
- Lyme disease
- Cytomegalovirus
- Myxedema/Thyroid disorder
- Idiopathic neuritis
Narrowing Down Common Causes Of Radiculopathy
Disc Herniation
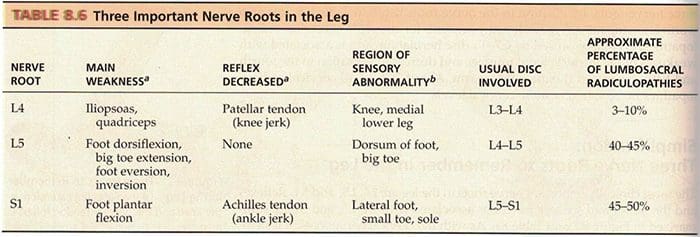
- Most commonly affected nerve roots are C6, C7, L5 & S1
Spinal Stenosis
- Lumbar stenosis may produce neurogenic claudication
- Pain & weakness with ambulation
- Cervical stenosis may present with mixed picture of radiculopathy and myelopathy due to long tract involvement
Trauma
- May cause compression, trauma or avulsion of the nerve roots
Diabetes
- More likely to cause a polyneuropathy, but mononeuropathy is possible
Herpes Zoster (Shingles)
- Most often on the trunk, accompanied by vesicular lesions in a single dermatome
- If pain persits past vesicular regression = post-herpetic neuralgia
Patient History Of Radiculopathy
- The patient will often complain of burning pain or tingling that radiates or shoots down an affected area in a dermatomal pattern.
- Sometimes patient will complain of motor weakness, however if onset is recent, there is often no motor involvement
Exam Of Radiculopathy
- Most often hypoesthesia in the affected dermatome level
- Best to evaluate for pain, as light touch can be difficult for these patient’s to distinguish
- Fasciculations and/or atrophy may be seen if radiculopathy is chronic, due to lower motor neuron being impinged
- Motor weakness may be seen in muscles innervated by the same root level
Orthopedic tests:
Straight-leg raise test (SLR)
- Pain between 10-60 degrees likely indicates nerve root compression
Well-leg raise/Crossed straight-leg raise test (WLR)
- If positive, 90% specificity for L/S nerve root compression
Valsalva Maneuver
- Positive if increase in radicular symptoms
Spinal Percussion
- Pain may indicate metastatic disease, abscess or osteomyelitis
Examinations: Merck Manual Professional
How To Test Reflexes
How To Do A Sensory Exam
How To Do A Motor Examination
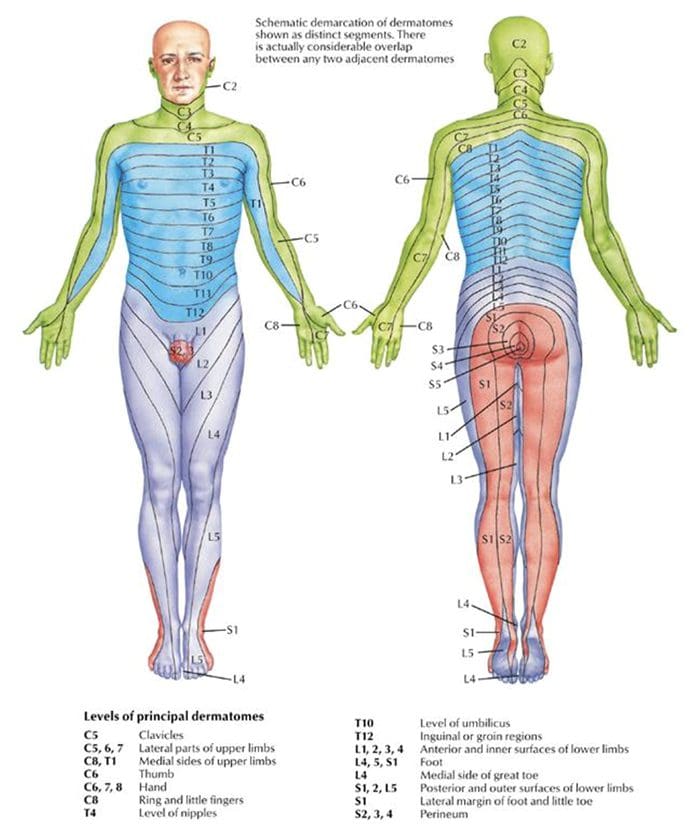
Dermatomes
Testing Cervical Nerve Roots
Testing Lumbosacral Nerve Roots
Specific Radiculopathy Patterns
T1 radiculopathy can cause Horner’s syndrome
- This is due to affect on cervical sympathetic ganglia
- Ptosis, miosis, anhidrosis
Below L1, radiculopathies can cause Cauda Equina syndrome
- Saddle anesthesia (sensory loss in S2-S5 distribution)
- Urinary retention or overflow incontinence
- Constipation, decreased rectal tone or fecal incontinence
- Loss of erectile function
- Must be referred for emergency care immediately to prevent permanent dysfunction
Other Patterns Of Neuropathy
Cape/Shawl distribution of symptoms
- Intramedullary lesion
- Syringomyelia
- Intramedullary tumor
- Central cord damage
Stocking and Glove Distribution of Symptoms
- Diabetes mellitus
- B12 deficiency
- Alcoholism/hepatitis
- HIV
- Thyroid dysfunction/myxedema
Cape/Shawl Pattern
- Intramedullary lesion such as tumor, syringomyelia or hyperextension injury in patient with C/S spondylosis
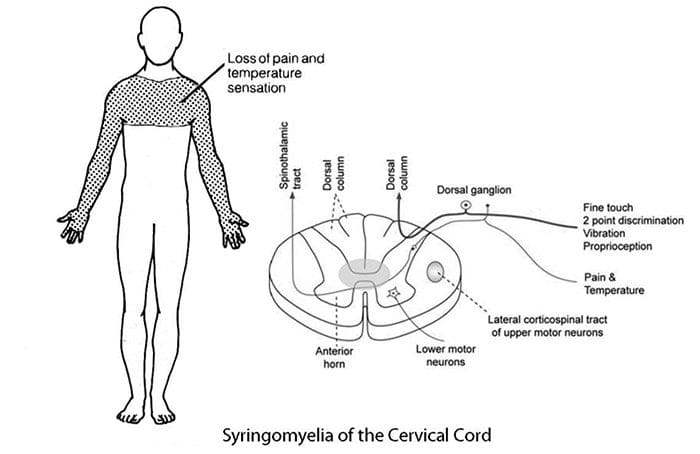
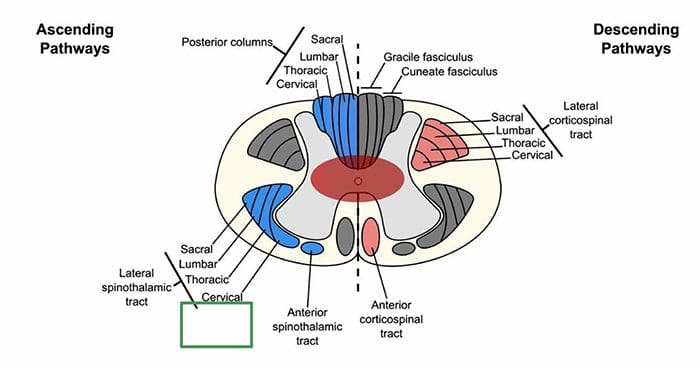
- Loss of pain and temp sensation in C/T dermatomes because of arrangement of lateral spinothalamic tract
Stocking & Glove Pattern
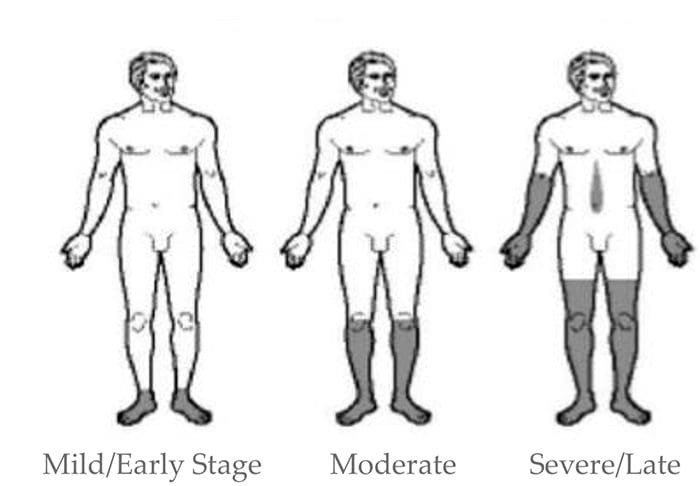
- Symmetrical polyneuropathy
- Feet/legs usually affected first, followed by hands/arms
- Vibration sensation in the smallest toes is usually the first thing lost and neuropathy progresses across foot to great toe and then upward through the ankle and leg, then hands, arms and finally trunk if sever
- Most likely cause of this distribution is diabetes mellitus, but other possible causes include B12 deficiency, alcoholism, HIV, chemotherapy treatment, thyroid dysfunction and multiple other causes
Diabetic Neuropathy
- Diabetic neuropathy often presents as a polyneuropathy but can also present as a mononeuropathy, usually with acute onset
- Most common in CN III, femoral and sciatic nerves
Demyelinating Neuropathies
- Acute inflammatory demyelinating polyneuropathy (Guillain-Barré syndrome)
- Chronic inflammatory demyelinating polyneuropathy
Guillain-Barré Syndrome (AIDP)
- Onset 1-2 weeks post viral infection
- Progressive weakness
- Loss of DTRs/areflexia
- Paresthesia in hands and feet
- More motor involvement than sensory
- Potential autonomic fiber involvement
- Elevated CSF protein
- EMG/NCV studies indicate demyelination
- May require treatment with plasmapheresis or IV Ig therapy
Chronic Inflammatory Demyelinating Polyneuropathy
- Appears similar to AIDP but does not follow infection
- Symptoms must be present for at least 8 weeks for this diagnosis to be considered
- Anti-inflammatory treatments may help
National University of Health Sciences Master of Science (MS) - Advanced Clinical Practice (ACP) MS ACP 551: Clinical Neurology © 2018
Sources
Blumenfeld, Hal. Neuroanatomy through Clinical Cases. Sinauer, 2002.Evans, Ronald C. Illustrated Orthopedic Physical Assessment. Mosby/Elsevier, 2009.
“Radial Nerve Entrapment: Background, Anatomy, Pathophysiology.” Medscape, 25 Oct. 2017, emedicine.medscape.com/article/1244110- overview#a8.
